Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Women with SLE and RA have an increased risk of delivering a preterm infant. However, the causes of these preterm births remain unknown. Some theories suggest that maternal inflammation induces preterm labor and/or rupture of membranes. We sought to identify what prompted each preterm delivery, as well as the mode of delivery among a cohort of patients with SLE and RA.
Methods: SLE patients meeting ACR and/or SLICC criteria and RA patients meeting ACR criteria were prospectively followed in a pregnancy registry. Pregnancy outcomes were collected from the patient and medical records. Preterm birth was defined as a birth <37 weeks gestation. Only singleton live births with a visit prior to 25 weeks gestation and data available on mode of delivery were included. At our institution, pregnancies in women with rheumatic diseases are routinely induced at 39 weeks for delivery, regardless of maternal complications. Differences between term and preterm births were determined by Fisher’s exact test.
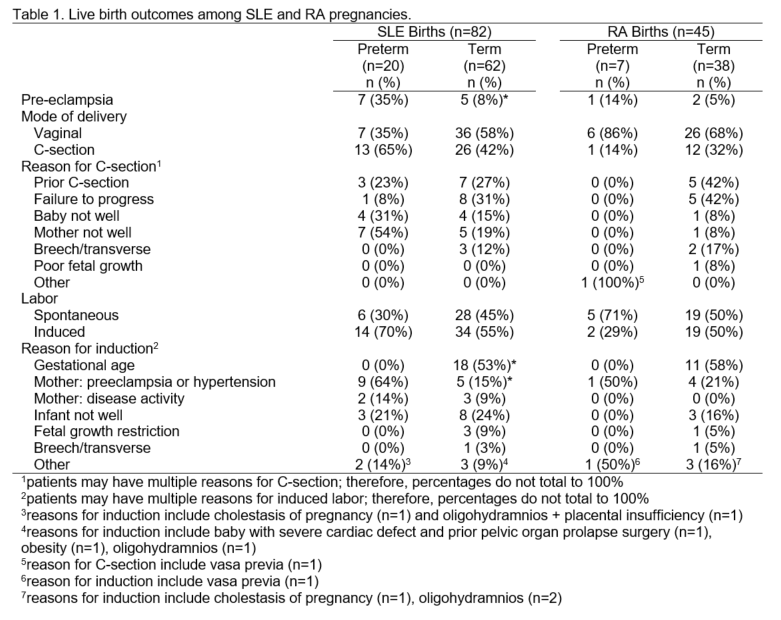
Results: Among 82 SLE live births, 46% of mothers were white and 46% were black, with a median maternal age of 30 years. Among 45 RA live births, 78% of mothers were white, with a median maternal age of 35 years. There were 20 preterm births (24%) among SLE pregnancies and 7 preterm births (16%) among RA pregnancies. While only 30% of preterm SLE births were spontaneous, 71% of preterm RA births were spontaneous. The frequency of C-section was greater in patients who had induced compared to spontaneous labor (65% vs. 24%, respectively, for SLE and 52% vs. 8%, respectively, for RA). Among SLE patients, preeclampsia and concern over the health of the mother were the primary drivers behind induced preterm labor and preterm C-sections (Table 1). Preeclampsia was diagnosed in 35% of preterm deliveries compared to 8% of term deliveries (p=0.002). Labor was induced in 70% of preterm births and 55% of term births. The reason for induction differed, however, with 64% of preterm births induced for maternal preeclampsia/hypertension compared to 15% of induced term births (p=0.001). In contrast, among women with RA, C-sections and preterm birth were both less frequent than in SLE, and labor was more often spontaneous. Half of term deliveries were induced, primarily for gestational age, although 21% of term births were induced due to maternal preeclampsia/hypertension and 16% were induced because the infant was not well.
Conclusion: Spontaneous preterm labor does not appear to be driving the high preterm birth rate among women with lupus. Instead, physician-directed labor induction to manage the risks of preeclampsia, placental insufficiency, and lupus activity prompts the majority of preterm births. These results suggest future research attention should focus on placental dysfunction and away from causes of spontaneous preterm labor.
To cite this abstract in AMA style:
Eudy AM, Neil L, Clowse MEB. Causes of Cesarean Section and Labor Induction in Systemic Lupus Erythematosus and Rheumatoid Arthritis Pregnancies [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/causes-of-cesarean-section-and-labor-induction-in-systemic-lupus-erythematosus-and-rheumatoid-arthritis-pregnancies/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/causes-of-cesarean-section-and-labor-induction-in-systemic-lupus-erythematosus-and-rheumatoid-arthritis-pregnancies/