Session Information
Session Type: Poster Session (Tuesday)
Session Time: 9:00AM-11:00AM
Background/Purpose: The human polyomaviruses, such as the BK and JC virus, are highly prevalent in humans but appear to cause clinical disease only in immunocompromised patients. BK virus (BKV) is the primary cause of tubulointerstitial nephritis and ureteral stenosis in kidney transplant recipients and hemorrhagic cystitis in bone marrow transplant recipients. Among transplant recipients, it has been hypothesized that the intensity of immune suppression, rather than the specific immunosuppressive agent used, determines the risk for BKV replication and progression to clinically significant disease.
Patients with autoimmune connective tissue diseases (CTD) like Systemic Lupus Erythematosus (SLE) and Rheumatoid arthritis (RA) have been shown to have increased polyomavirus levels in blood and urine. The treatment for these autoimmune diseases include medications like corticosteroids and disease modifying anti-rheumatic drugs (DMARDS), including biologics and cytotoxic agents which have been shown to increase the frequency of virus reactivation/excretion in prior studies. The purpose of this study was to determine the prevalence of BK virus in the blood and its excretion in urine in immunosuppressed patients with CTDs. We hypothesized that subjects on DMARDS plus steroids would have the highest prevalence of BKV viremia and viruria.
Methods: Sixty-six patients with CTD on various immunosuppressive regimens (including Prednisone, Mycophenolate Mofetil, Methotrexate, Leflunomide, Azathioprine, Sulfasalazine, Hydroxychloroquine, Tumor necrosis factor inhibitors, Tocilizumab, Rituximab, Cyclophosphamide) and control subjects were enrolled after informed consent was obtained. Urine and serum specimens were collected at each clinic visit and analyzed qualitatively and quantitatively for BK virus by PCR. Subjects’ demographic data, diagnosis and medications were recorded at the time of each clinic visit. The frequency of BKV viruria and viremia was compared for clinical and demographic factors using Chi-square analysis. Multivariate analysis is planned once the study population reaches 100.
Results: The average age of study subjects was 53.5 +/- 12.4 years and 46 (69.7%) were African-American. Fifty-six (84.8%) subjects were female. Twenty subjects had RA, 15 had SLE, 31 had other diagnosis like Psoriatic arthritis, myositis, scleroderma. Serum and Urine specimens were collected from study subjects at 239 clinical visits. 155 (64.8%) of 239 urine specimens and 106 (45.1%) of 239 serum specimens were positive for BKV. There was no difference in the frequency of BKV viremia or viruria based on the subject’s diagnosis (RA (49.2% and 62.9%) vs SLE (43.1% and 68.4%) vs other (43.6% and 69.6%)) Figure 1, or medication regimen (none vs. steroids vs. DMARDS vs. DMARDS + steroids) Figure 2.
Conclusion:
Contrary to our hypothesis, there was no statistical difference between the frequency of BK-positive serum or urine by medication group. Likewise, there was no statistical difference in the frequency of BKV viremia or viruria by subject’s CTD diagnosis. These data suggest that immunologic control of BKV viremia and viruria may be dysregulated in CTD, independent of immunosuppressive regimens.
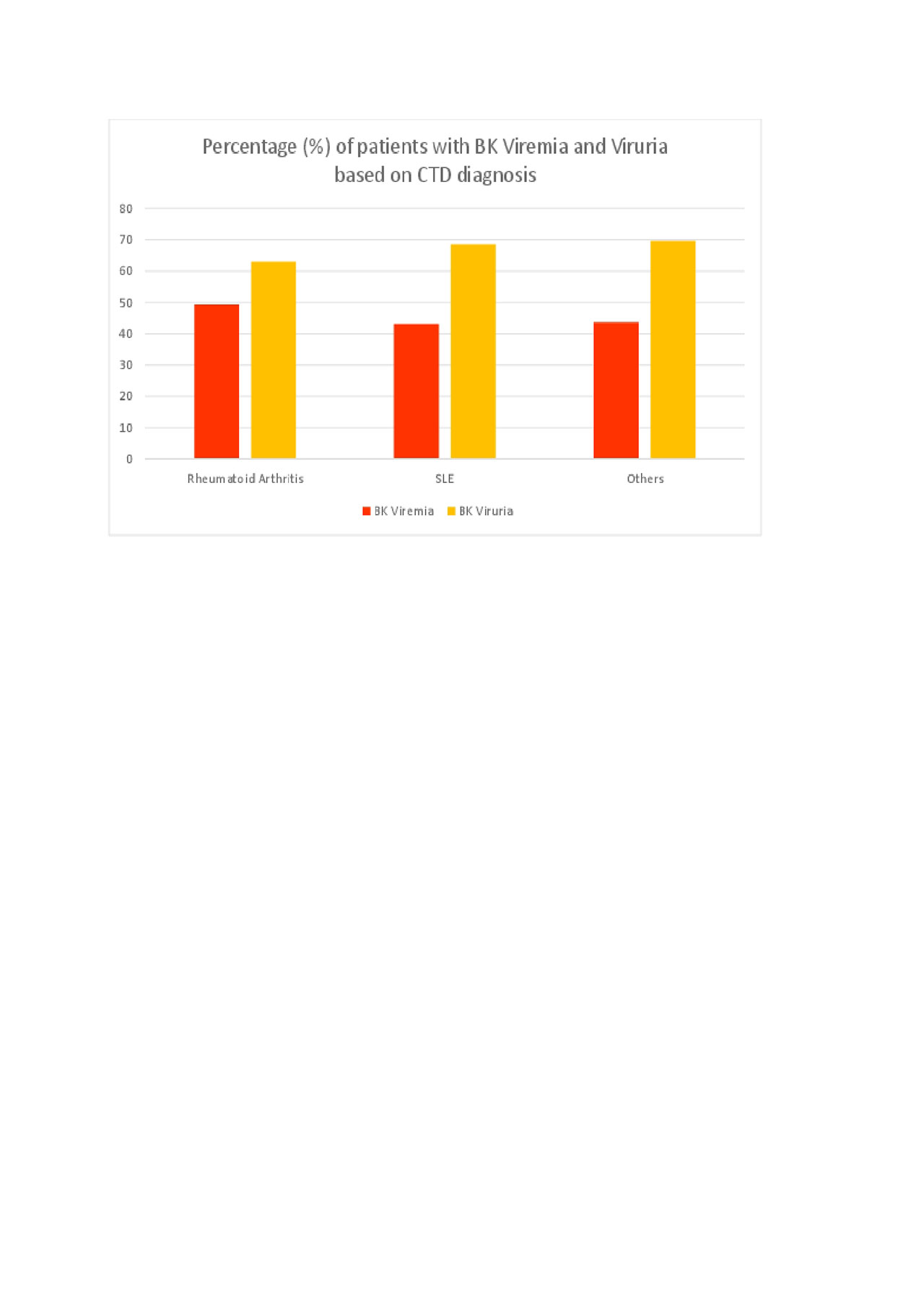
BK Virus Figure 1
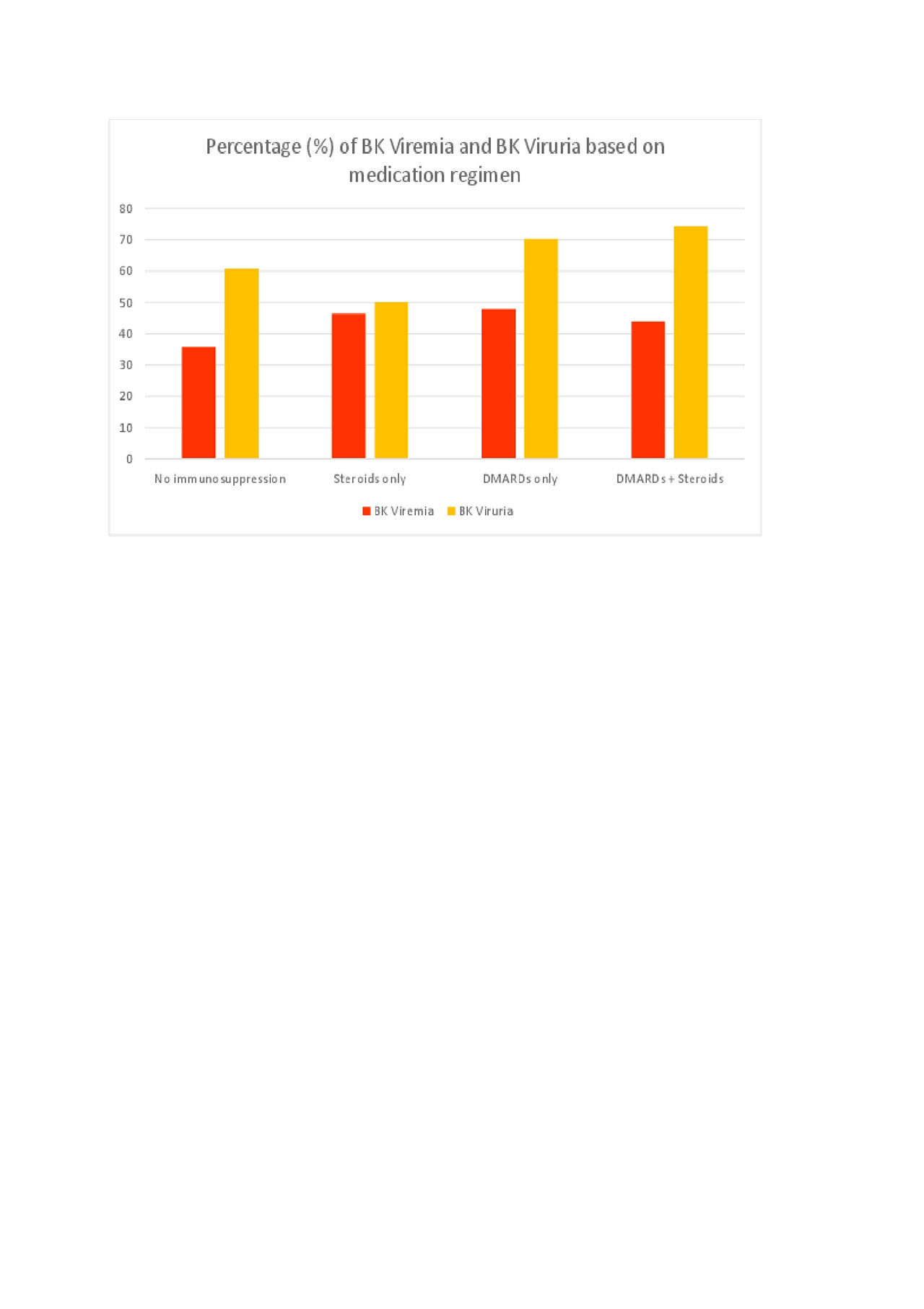
BK Virus Figure 2
medication regimen
To cite this abstract in AMA style:
Katikaneni M, Davis M, Smith C, Vanchiere J. BK Polyomavirus Viremia and Viruria in Patients with Autoimmune Connective Tissue Diseases: Impact of Immunosuppressants [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/bk-polyomavirus-viremia-and-viruria-in-patients-with-autoimmune-connective-tissue-diseases-impact-of-immunosuppressants/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/bk-polyomavirus-viremia-and-viruria-in-patients-with-autoimmune-connective-tissue-diseases-impact-of-immunosuppressants/