Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Axial spondyloarthritis (axSpA) is a chronic rheumatic disease requiring optimal management. Assessment of SpondyloArthritis international Society ≥40% improvement (ASAS40) and ASAS partial remission (ASAS PR) are stringent outcomes in trials, while in clinical practice the focus is on sustained remission (inactive disease [ID]) or low disease activity (LDA) according to axSpA Disease Activity Score (ASDAS; < 1.3 and < 2.1, respectively). Maintenance of response is an internationally recommended target for patient (pt) care.1
Bimekizumab (BKZ) is a monoclonal IgG1 antibody that selectively inhibits IL-17F in addition to IL‑17A. BKZ demonstrated sustained clinical efficacy to Week (Wk) 52 in pts across the full disease spectrum of axSpA in the phase 3 studies BE MOBILE 1 and 2.2 This analysis assessed the maintenance of response to BKZ over 2 years in the open-label extension (OLE) of those studies.
Methods: BE MOBILE 1 (NCT03928704) and 2 (NCT03928743) comprised a 16-wk double-blind period followed by a 36-wk maintenance period in pts with non-radiographic (nr-) and radiographic (r-)axSpA, respectively.2 Pts were randomized to receive subcutaneous BKZ 160 mg every 4 wks (Q4W) or placebo (PBO); from Wk 16, all received BKZ. At Wk 52, eligible pts could enroll into BE MOVING (OLE; NCT04436640).
The proportions of pts achieving ASAS40, ASAS PR, ASDAS LDA and ASDAS ID to Wk 104 were assessed among BKZ‑randomized pts who achieved each respective outcome at Wk 16, pooled across studies. Presented data use non-responder imputation (NRI), multiple imputation (MI) and worst category imputation (WCI; ASDAS only). Observed case (OC) data are also reported.
Treatment-emergent adverse events (TEAEs) to Wk 104 are reported for pts who received ≥1 BKZ dose, including pts who switched from PBO to BKZ at Wk 16.
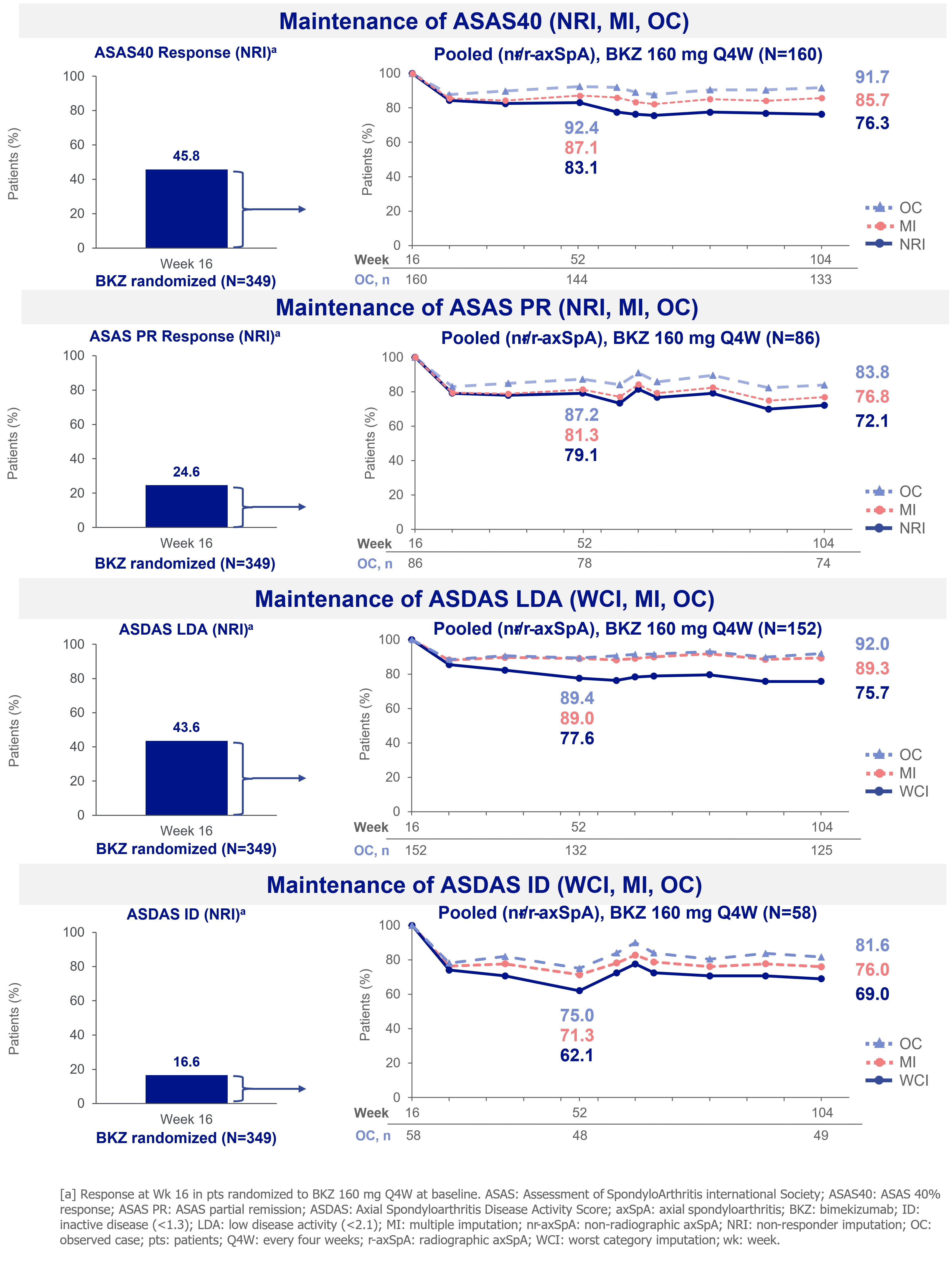
Results: A total of 128 and 221 pts were randomized to BKZ in BE MOBILE 1 and 2, respectively (N=349). High proportions of pts who achieved a response at Wk 16 maintained their responses at Wk 104 (Figure).
At Wk 16, 160 (45.8%) pts achieved ASAS40; this increased to 180 (51.6%) pts at Wk 104 (NRI). Of pts who achieved ASAS40 at Wk 16, 85.7% maintained this response at Wk 104 (MI). At Wk 16, ASAS PR was achieved by 86 (24.6%) pts; this increased to 100 (28.7%) pts at Wk 104 (NRI). Of pts who achieved ASAS PR at Wk 16, 76.8% also achieved this outcome at Wk 104 (MI; Figure).
ASDAS LDA was achieved by 152 (43.6%) pts at Wk 16; this increased to 172 (49.3%) at Wk 104 (NRI). Of pts who achieved ASDAS LDA at Wk 16, 89.3% also achieved this outcome at Wk 104 (MI). ASDAS ID was achieved by 58 (16.6%) pts at Wk 16; this increased to 88 (25.2%) at Wk 104 (NRI). Of pts who achieved ASDAS ID at Wk 16, 76.0% achieved this outcome at Wk 104 (MI; Figure).
Through Wk 104, 514/574 (89.5%; exposure-adjusted incidence rate per 100 pt-years [EAIR/100 PY]: 141.9) pts had ≥1 TEAE whilst receiving BKZ; 72 (12.5%; EAIR/100 PY: 5.4) had serious TEAEs. 39 (6.8%; EAIR/100 PY: 2.8) pts discontinued BKZ due to TEAEs.
Conclusion: Using the most critical statistical methodology (NRI or WCI; MI), BKZ maintained stringent clinical responses from Wk 16 to Wk 104 in axSpA. No new safety signals were observed.
References: 1. Ramiro S. Ann Rheum Dis 2023;82:19–34; 2. Baraliakos X. Ann Rheum Dis. 2024;83:199–213.
To cite this abstract in AMA style:
Proft F, van der Heijde D, Schwartzman S, Ermann J, Marten A, Massow U, Stojan G, Taieb V, Voiniciuc D, van Tubergen A, Navarro Compán V, Baraliakos X. Bimekizumab Maintained Stringent Clinical Responses over 2 Years in Patients with Axial Spondyloarthritis: Results from Two Phase 3 Studies [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/bimekizumab-maintained-stringent-clinical-responses-over-2-years-in-patients-with-axial-spondyloarthritis-results-from-two-phase-3-studies/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/bimekizumab-maintained-stringent-clinical-responses-over-2-years-in-patients-with-axial-spondyloarthritis-results-from-two-phase-3-studies/