Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: PsA is a chronic disease, and patients (pts) can experience loss of response with sustained therapy; therefore, assessing long-term maintenance of response in pts achieving early treatment targets is important.1 Bimekizumab (BKZ), a monoclonal IgG1 antibody that selectively inhibits IL-17F in addition to IL-17A, has demonstrated clinically meaningful improvements in efficacy outcomes to Week (Wk) 16, that were sustained to Wk 52, in pts with PsA.2,3 Here, we report the proportion of Wk 16 responders maintaining their response in joint, skin, and composite efficacy outcomes up to 2 years in BKZ-treated pts with PsA.
Methods: Two phase 3 studies assessed subcutaneous BKZ 160 mg every 4 weeks in pts with PsA: BE OPTIMAL (biologic DMARD [bDMARD]-naïve; NCT03895203) and BE COMPLETE (TNF inhibitor inadequate response/intolerance [TNFi-IR]; NCT03896581); both were placebo-controlled to Wk 16. BE OPTIMAL Wk 52 and BE COMPLETE Wk 16 completers were eligible for BE VITAL (open-label extension; NCT04009499). Efficacy data are reported for pts randomized to BKZ at baseline (BL); safety data are reported for all BKZ-treated pts.
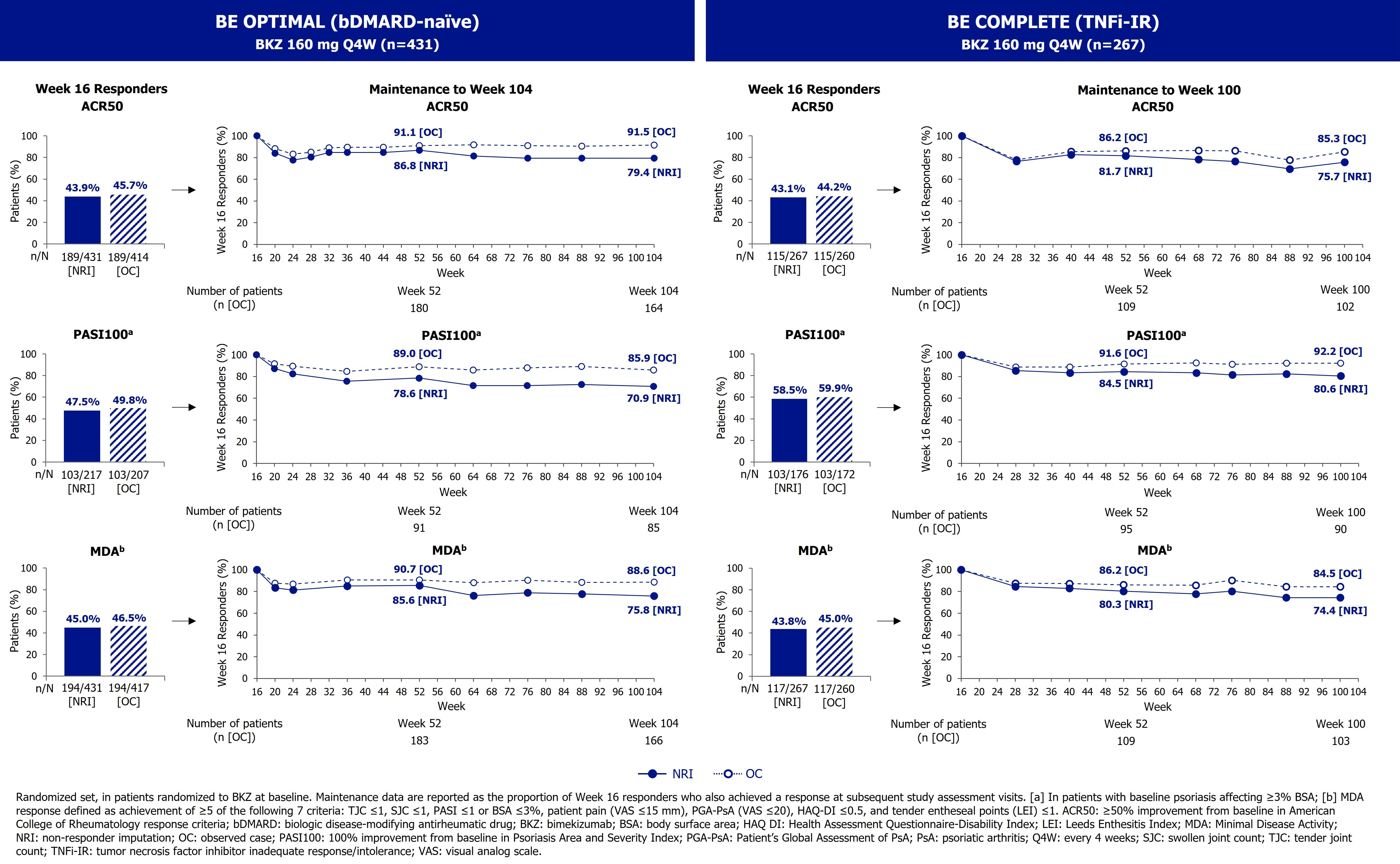
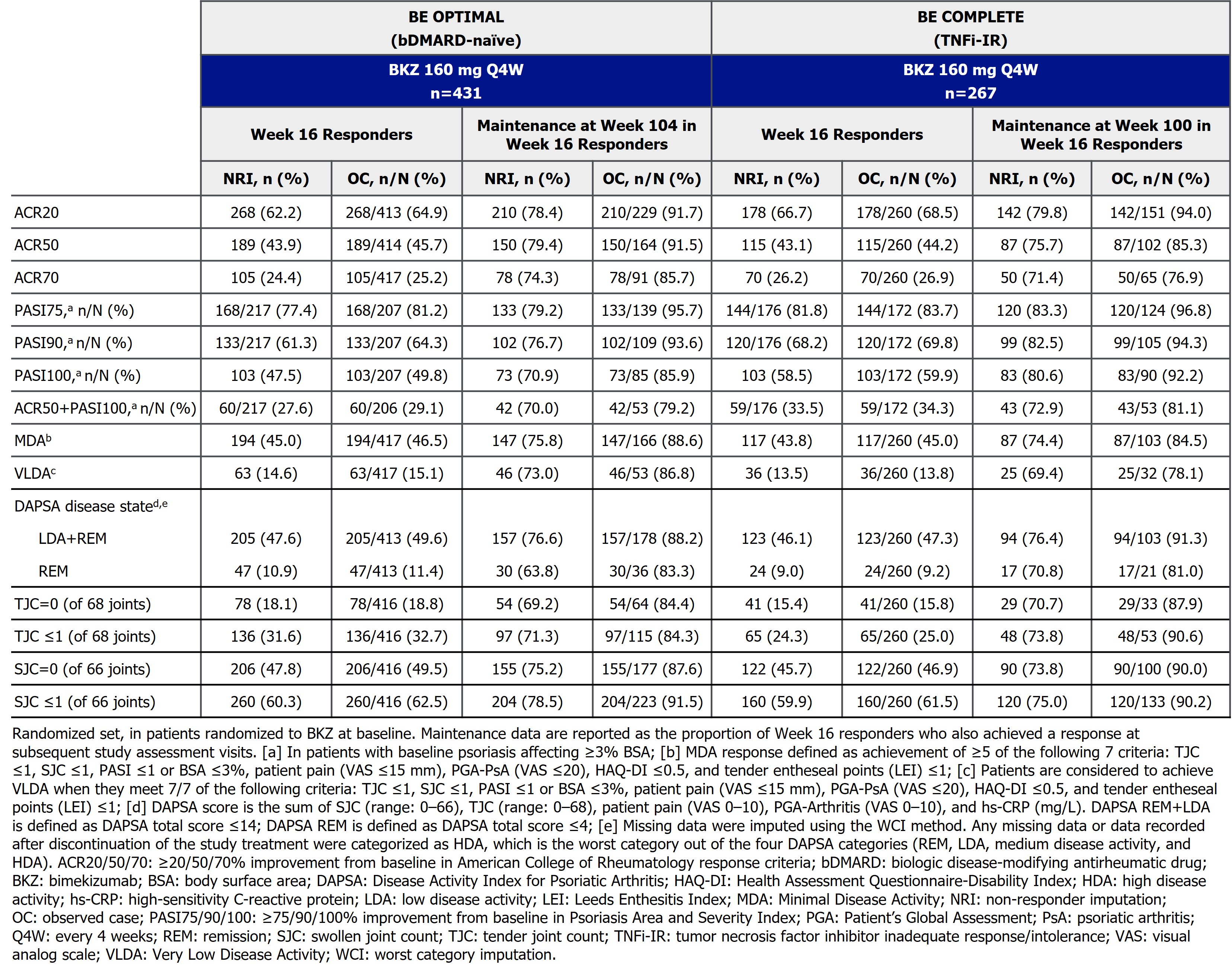
Maintenance of response is reported as the proportion of Wk 16 responders who were responders at Wk 104/100 (BE OPTIMAL/BE COMPLETE). Efficacy outcomes include ACR20/50/70, Psoriasis Area and Severity Index (PASI)75/90/100, Minimal/Very Low Disease Activity (MDA/VLDA), and Disease Activity Index for PsA (DAPSA) remission or low disease activity responses (REM ≤4; REM+LDA ≤14); these are reported here to Wk 104 in BE OPTIMAL and Wk 100 in BE COMPLETE. Data are reported as observed case or using non-responder or worst category imputation. Exposure-adjusted incidence rates per 100 pt-years (EAIR/100 PY) are reported to Wk 104 for both bDMARD-naïve and TNFi-IR pts.
Results: Of BKZ-randomized pts, 359/431 (83.3%) bDMARD-naïve and 215/267 (80.5%) TNFi-IR pts completed Wk 104/100.
High proportions of pts achieving ACR50, PASI100, and MDA at Wk 16 maintained responses at Wk 104/100 (Figure, Table). At Wk 16, 189 (43.9%) bDMARD-naïve and 115 (43.1%) TNFi-IR pts achieved ACR50; of those, 150 (79.4%) bDMARD-naïve and 87 (75.7%) TNFi-IR pts maintained response at Wk 104/100. Similarly, for pts with BL psoriasis affecting ≥3% body surface area, 103/217 (47.5%) bDMARD-naïve and 103/176 (58.5%) TNFi-IR pts achieved PASI100 at Wk 16; of those, 73 (70.9%) bDMARD-naïve and 83 (80.6%) TNFi-IR pts maintained response at Wk 104/100. MDA was achieved by 194 (45.0%) bDMARD-naïve and 117 (43.8%) TNFi-IR pts at Wk 16; of those, 147 (75.8%) bDMARD-naïve and 87 (74.4%) TNFi-IR pts maintained response at Wk 104/100. Similar results were observed for other joint, skin, and composite efficacy outcomes at Wk 104/100 (Table).
To Wk 104, the EAIR/100 PY for BKZ-treated pts with ≥1 treatment-emergent adverse event was 179.9 in bDMARD-naïve and 100.3 in TNFi-IR pts.
Conclusion: BKZ demonstrated robust maintenance of response at 2 years in both bDMARD-naïve and TNFi-IR pts with PsA who responded to BKZ treatment at Wk 16. The safety profile was consistent with previous reports.2,3
References: 1. Boehncke WH. Am J Clin Dermatol 2013;14:377–88; 2. Ritchlin CT. Ann Rheum Dis 2023;82:1404–14; 3. Coates LC. RMD Open 2024;10:e003855.
To cite this abstract in AMA style:
Walsh J, Merola J, Ritchlin C, Tanaka Y, Favalli E, McGonagle D, Thaçi D, Ink B, Bajracharya R, Coarse J, Tillett W. Bimekizumab Maintained Efficacy Responses in Patients with Active Psoriatic Arthritis: Up to 2-Year Results from Two Phase 3 Studies [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/bimekizumab-maintained-efficacy-responses-in-patients-with-active-psoriatic-arthritis-up-to-2-year-results-from-two-phase-3-studies/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/bimekizumab-maintained-efficacy-responses-in-patients-with-active-psoriatic-arthritis-up-to-2-year-results-from-two-phase-3-studies/