Session Information
Date: Monday, November 13, 2023
Title: (1412–1441) Spondyloarthritis Including Psoriatic Arthritis – Treatment Poster II: SpA
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
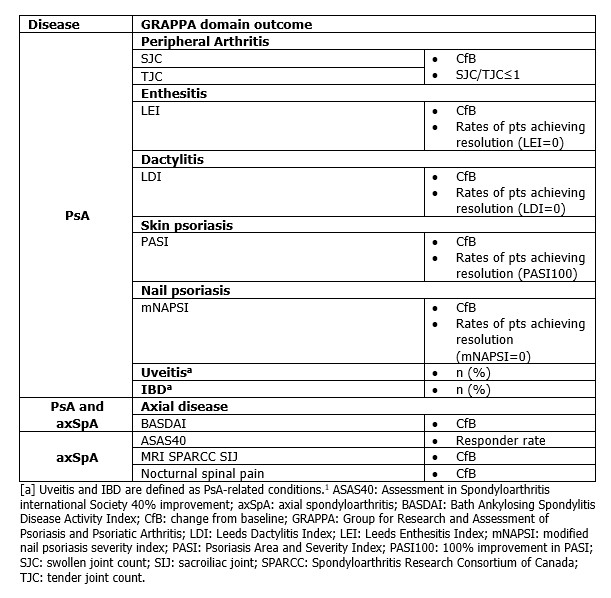
Background/Purpose: The Group for Research and Assessment of Psoriasis and PsA (GRAPPA) domain‑based treatment recommendations for PsA focus on six key domains: peripheral arthritis, axial disease, enthesitis, dactylitis, skin psoriasis, and nail psoriasis, and PsA-related conditions: uveitis and IBD.1Bimekizumab (BKZ), a monoclonal IgG1 antibody that selectively inhibits IL‑17F in addition to IL‑17A, has demonstrated superior clinical efficacy vs placebo (PBO) to Week (Wk) 16 in phase 3 clinical trials of patients (pts) with PsA.2,3 In pts with psoriasis, superior skin domain efficacy has been demonstrated versus secukinumab (IL-17A inhibitor), ustekinumab (IL-12/23 inhibitor), and adalimumab (TNF-α inhibitor [TNFi]).4–6 The objective of this analysis is to show BKZ efficacy across GRAPPA core domains to Wk 52 from two phase 3 trials in PsA, with axial domain outcomes from two phase 3 trials in axial spondyloarthritis (axSpA).
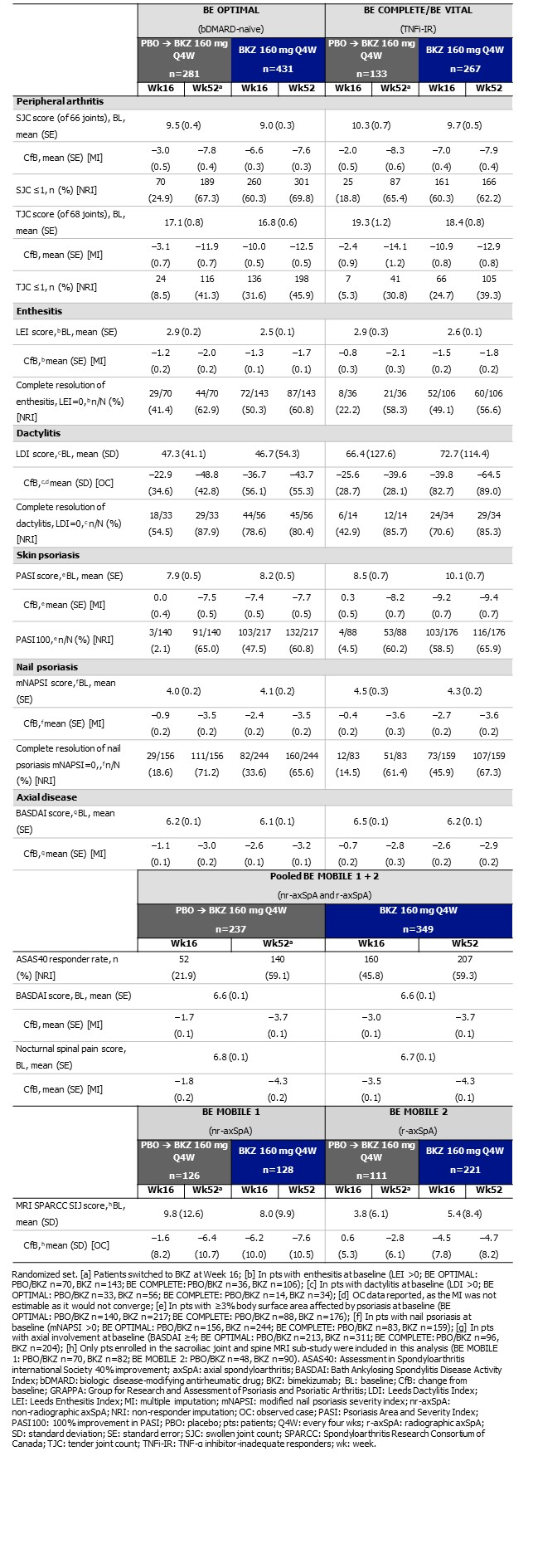
Methods: Included pts were randomized to receive subcutaneous BKZ 160 mg or PBO every 4 wks (Q4W) in BE OPTIMAL (NCT03895203; biologic DMARD‑naïve pts with PsA), BE COMPLETE (NCT03896581; pts with PsA who were TNFi‑inadequate responders [TNFi‑IR]), BE MOBILE 1 (NCT03928704; non‑radiographic axSpA) and BE MOBILE 2 (NCT03928743; radiographic axSpA, i.e. ankylosing spondylitis). BE OPTIMAL included a reference arm (adalimumab 40 mg Q2W) to Wk 52; data not shown.2,3,7 From Wk 16, all PBO-randomized pts received BKZ 160 mg Q4W to Wk 52 (PBO/BKZ). Wk 16 completers from BE COMPLETE were eligible to enter BE VITAL (NCT04009499; open‑label extension). Outcomes are reported by GRAPPA domain (Table 1). Missing data are imputed using non‑responder and multiple imputation (NRI; MI) for binary and continuous outcomes, or reported using observed case (OC).
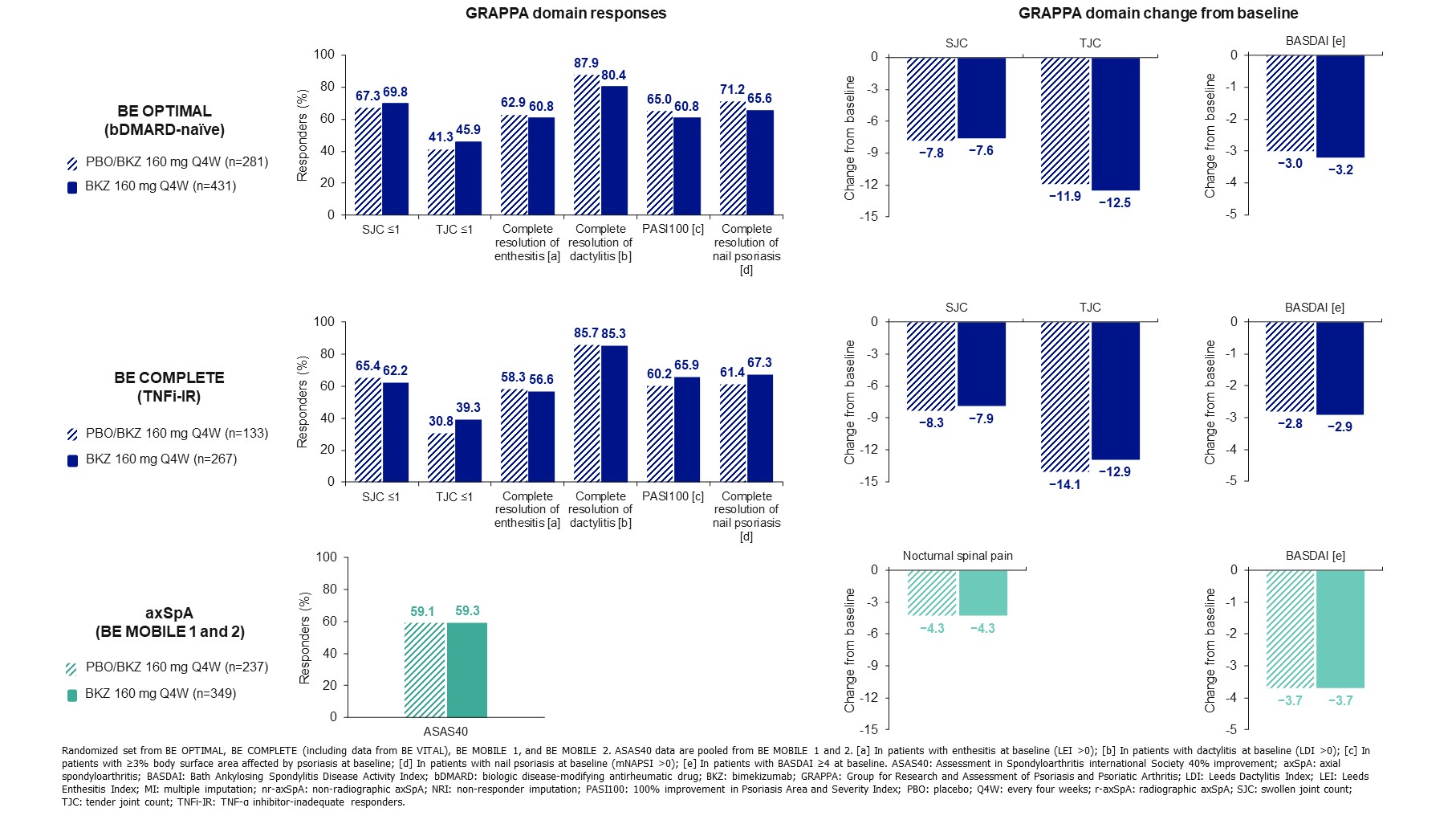
Results: Wk 52 completion was high (BE OPTIMAL: 770/852 [90.4%], BE COMPLETE: 347/400 [86.8%], BE MOBILE 1: 220/254 [86.6%], BE MOBILE 2: 298/332 [89.8%]). Baseline demographics and disease characteristics were previously reported.2,3,7 Across all GRAPPA domains, improvements from Wk 16 were sustained at Wk 52 in BKZ‑treated pts across all studies (Table 2). Individual domain responses were generally consistent between bDMARD‑naïve and TNFi-IR pts (Figure). Results from BE MOBILE 1 and 2 demonstrated BKZ efficacy in pts with axSpA (Table 2, Figure) and were suggestive of efficacy for axial disease in PsA.1 Responses were generally consistent between BKZ and PBO/BKZ pts at Wk 52 (Figure). To Wk 52, there were no instances of uveitis (BE OPTIMAL; BE COMPLETE). 2 (0.2%) pts in BE OPTIMAL had definite adjudicated IBD; no pts had adjudicated IBD in BE COMPLETE.
Conclusion: Treatment with BKZ resulted in robust and sustained improvements across GRAPPA domains with low rates of IBD and no uveitis to Wk 52 for both bDMARD‑naïve and TNFi‑IR pts with PsA; results from pts with axSpA support efficacy in the axial domain.
References:1. Coates LC. Nat Rev Rheumatol 2022;18:465–79; 2. McInnes IB. Lancet 2023;401:25–37; 3. Merola JF. Lancet 2023;401:38–48; 4. Reich K. N Engl J Med 2021;385:142–52; 5. Reich K. Lancet 2021;397:487–98. 6. Warren RB. N Engl J Med 2021;385:130–41; 7.Van der Heijde D. Ann Rheum Dis 2023;82:515–26.
To cite this abstract in AMA style:
Merola J, Mease P, Deodhar A, Ink B, Fleurinck C, Bajracharya R, Coarse J, Coates L. Bimekizumab Impact on Core Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) Domains for Patients with Psoriatic Arthritis: 52-Week Results from Four Phase 3 Studies [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/bimekizumab-impact-on-core-group-for-research-and-assessment-of-psoriasis-and-psoriatic-arthritis-grappa-domains-for-patients-with-psoriatic-arthritis-52-week-results-from-four-phase-3-studies/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/bimekizumab-impact-on-core-group-for-research-and-assessment-of-psoriasis-and-psoriatic-arthritis-grappa-domains-for-patients-with-psoriatic-arthritis-52-week-results-from-four-phase-3-studies/