Session Information
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: Many combat veterans experience unexplained symptoms with long-term disability including chronic pain, irritability, headaches, fatigue, behavioral health conditions, and memory difficulty. These invisible wounds were poorly described when the term “shell shock” was first used in WWI. Half a century later, Gulf War syndrome encompassed many characteristic symptoms of fibromyalgia (FMS), irritable bowel syndrome, and chronic fatigue. Following the wars in Iraq and Afghanistan, onset of FMS and post traumatic stress disorder (PTSD) in active duty and veteran populations was extensively studied. Our understanding deepened with improved knowledge of neurobiology and trauma. However, a clear understanding of the risk factors and interplay between these disorders was lacking. As PTSD and chronic pain syndromes often occur in both combat and non-combat veterans, we hypothesized that deployment was not the primary factor. Behavioral health disorders such as PTSD and musculoskeletal pain such as FMS are leading reasons for premature discharge from active duty. Therefore, understanding risk factors for these disorders is necessary to mitigate the impact on military readiness. Our objective is to determine whether deployment history, history of deployment to a combat zone, and history of deployment to a combat zone during times of high casualty rates were associated with development of FMS.
Methods: A total of 2423 active-duty patients were included. FMS was significantly associated with female sex, sleep apnea, depression, anxiety, PTSD, and deployment to a combat zone during times of peak combat casualties (identified as Iraq from 2003-2008, and Afghanistan from 2009-2013). When controlled for dependent variables in multivariate analysis, deployment to a combat zone during times of peak combat casualties remained significantly associated with FMS. Whereas deployment during other time periods was not associated with the development of FMS.
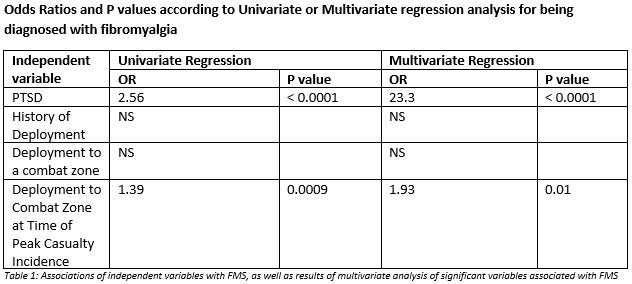
Results: A total of 2423 active duty patients were included. FMS was the most common primary rheumatologic diagnosis (27.8%). FMS was significantly associated with female sex, sleep apnea, depression, anxiety, PTSD, and deployment to a combat zone during times of peak combat casualties (identified as Iraq from 2003-2008, and Afghanistan from 2009-2013). When the eight variables which were significant in the univariate analyses were included in multivariate analysis, deployment to a combat zone during times of peak combat casualties remained significantly associated with FMS.
Conclusion: Deployment to a combat zone during times of peak casualty incidence was independently associated with the presence of FMS. Further, FMS and deployment during times of peak casualty incidence were both independently associated with the presence of PTSD. This suggests a notable association between deployment at a time of high casualties, FMS, and PTSD. It also underscores the risk that combat adds to development of FMS, as deployment to a combat zone at any time was not significantly associated with FMS. These findings emphasize the unique risk that military members encounter in developing FMS, and will aid in improving the design of future trials on FMS in active duty service members.
To cite this abstract in AMA style:
Dizmang J, Tofferi J. Association of Fibromyalgia, PTSD and Combat Deployments in Active Duty Military [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/association-of-fibromyalgia-ptsd-and-combat-deployments-in-active-duty-military/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/association-of-fibromyalgia-ptsd-and-combat-deployments-in-active-duty-military/