Session Information
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Systemic lupus erythematosus (SLE) is recognized as an independent risk factor for cardiovascular disease (CVD). This study aimed to determine which cardiovascular risk assessment tool amongst the QRISK2, QRISK3, Framingham (FRS), Modified FRS (mFRS) or SLE Cardiovascular Risk Equation (SLECRE) best predicts CVD in SLE. QRISK3, mFRS and SLECRE are CVD risk assessment tools that consider SLE in risk prognosticating patients.
Methods: Single-centre analyses on prospectively collected data of 1887 SLE patients were performed to compute 10-year CVD risk scores for each tool. Tools’ scores were evaluated against CVD development at or within ten years for cases (CVD events) and controls (no CVD events). For cases, the index date for risk score calculation was chosen 10 years, or as close to 10 years as possible prior to the CVD event. Similarly, for controls, risk scores were calculated as close to 10 years as possible prior to the most recent clinic appointment. Proportions of patients classified as low risk (< 10%), median risk (10-20%) and high risk ( >20%) of developing CVD according to each tool were determined. Sensitivity, specificity, positive/negative predictive values and c-statistics of these tools were analyzed.
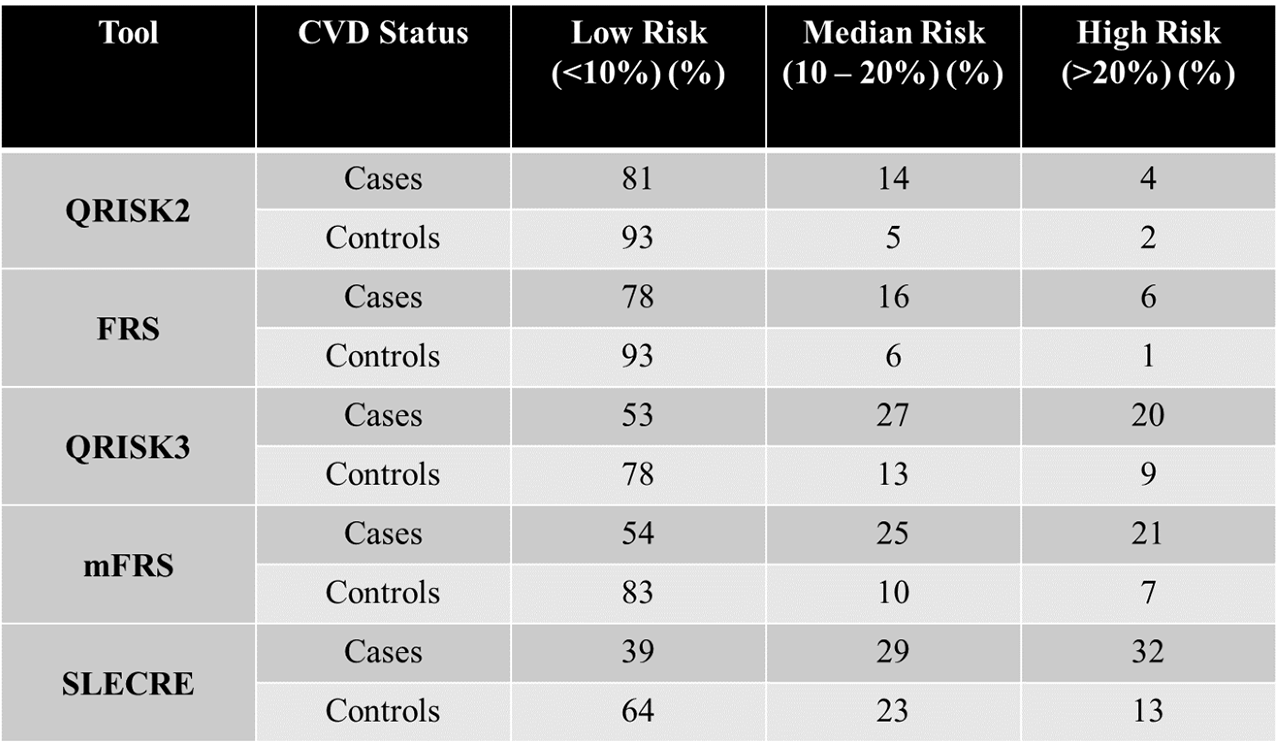
Results: 232 total CVD events were seen in the cohort including myocardial infarction, stroke, transient ischemic attack, heart failure and CVD death. QRISK2 and FRS performances were similar, while the QRISK3 and mFRS performances were similar. The SLECRE classified the highest number of patients as median-high risk (Table 1). The sensitivities and specificities are as follows for each tool: QRISK2 (19%, 93%), FRS (22%, 93%), mFRS (46%, 83%), QRISK3 (47%, 78%), SLECRE (61%, 63%), respectively. The tools were similar in negative predictive value, ranging from 89% (QRISK2) to 92% (SLECRE). The FRS and mFRS had the greatest c-statistics, both equaling 0. 73, demonstrating the greatest predictive accuracy amongst the tools, while the QRISK3 and SLECRE had the lowest (0. 67).
Conclusion: While the mFRS performance was superior to the FRS, the QRISK3 did not outperform the mFRS. Although the SLECRE had the highest sensitivity, it had the lowest specificity, demonstrated by grouping the most cases and controls in the median-high risk category. Several factors are important to consider when deciding which risk assessment tools to utilize clinically: ease of use, sensitivity/specificity, and laboratory data accessibility. Thus, the mFRS continues to be a practical tool with a simple, intuitive scoring system appropriate for the ambulatory clinic setting based on the initial weighting of the FRS while adjusting for SLE.
To cite this abstract in AMA style:
Sivakumaran J, Harvey P, Omar A, Urowitz M, Gladman D, Anderson N, Su J, Touma Z. Assessment of the QRISK2, QRISK3, SLE Cardiovascular Risk Equation, Framingham and Modified Framingham Risk Calculators as Predictors of Cardiovascular Disease Events in Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/assessment-of-the-qrisk2-qrisk3-sle-cardiovascular-risk-equation-framingham-and-modified-framingham-risk-calculators-as-predictors-of-cardiovascular-disease-events-in-systemic-lupus-erythematosus/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/assessment-of-the-qrisk2-qrisk3-sle-cardiovascular-risk-equation-framingham-and-modified-framingham-risk-calculators-as-predictors-of-cardiovascular-disease-events-in-systemic-lupus-erythematosus/