Session Information
Session Time: 5:00PM-6:00PM
Background/Purpose: Recent research suggests that multidimensional area-level indicators, including the Social Vulnerability Index (SVI), Area Deprivation Index (ADI) and Childhood Opportunity Index (COI), associate with childhood-onset systemic lupus erythematosus (cSLE) outcomes in primarily urban populations. However, to date, there are no studies that have assessed the utility of multidimensional area level indicators in children with cSLE living in rural areas. The goal of this study is to estimate relationships between neighborhood conditions and disease activity in children with cSLE who live in a mixed rural and urban setting. We hypothesized that patients with cSLE living in areas with higher social vulnerability and area-level deprivation have increased lupus activity.
Methods: We retrospectively evaluated electronic health record data for pediatric patients with cSLE across three pediatric rheumatology clinics at a single center between January 1, 2020 and December 31, 2024. We included patients with a diagnosis of cSLE before 18 years of age, a residential address within South Carolina, and excluded PO box addresses. Chart reviews were conducted to collect demographic data and addresses were linked to census tract-level indicators, including ADI, SVI and COI, ranked at state and national levels. We assessed each patient’s SLEDAI-2K score at their first clinic or hospital encounter associated with a SLE diagnosis.
Results: Baseline characteristics have been established for a cohort of 85 children with cSLE. The majority of patients identified as Black 65 (79%), followed by White 11 (13%), Latino/a 6 (6%), Asian 1 (1%), and Other 1 (1%). The cohort was predominantly female (87.1%), with a mean age at diagnosis of 13.0 years (range: 6–17). The mean SLEDAI-2K at the initial encounter was 14.4 (range: 0-38). There was no statistically significant relationship found between any of the MDIs at the state level (AVI, SVI, and COI) and lupus disease activity, as evidenced by initial SLEDAI-2K score and attainment of LLDAS by the end of the study period. There was no relationship between state level AVI, SVI and COI on development of lupus nephritis and there was no relationship between state level AVI and SVI on development of CNS lupus. However, patients in high COI areas had lower odds of developing CNS lupus.
Conclusion: Most participants included in the cohort, lived in areas with low state ranked SVI scores, high deprivation scores and low opportunity. Despite the cohort’s residence in predominantly deprived and low-opportunity areas, these indicators did not appear to predict lupus severity at first presentation to care or development of complications from lupus. No significant association between any of the MDI’s at the state level (AVI, SVI and COI) and the SLEDAI-2K score or achieved of LLDAS during the study period was found. The study also found no significant association between the MDIs at the state level (AVI, SVI and COI) on complications of lupus, specifically lupus nephritis, however, the study did show that patients in high COI areas had lower odds of developing CNS lupus.
Map 1 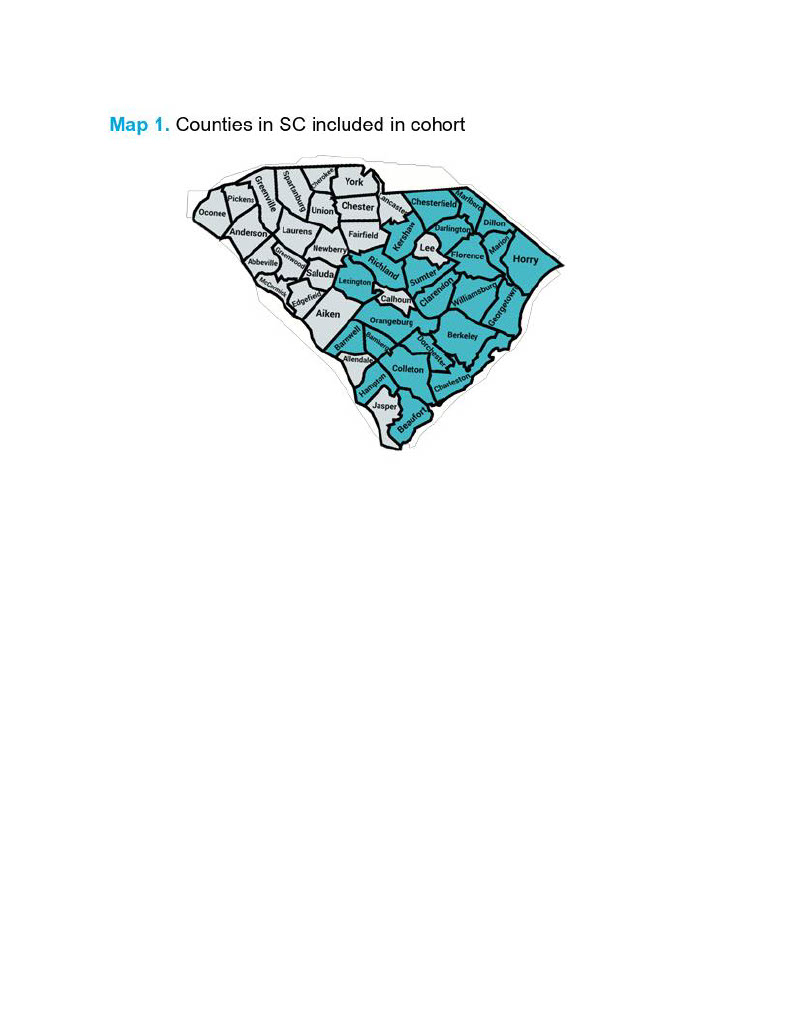 Counties in SC included in cohort
Counties in SC included in cohort
Table 1 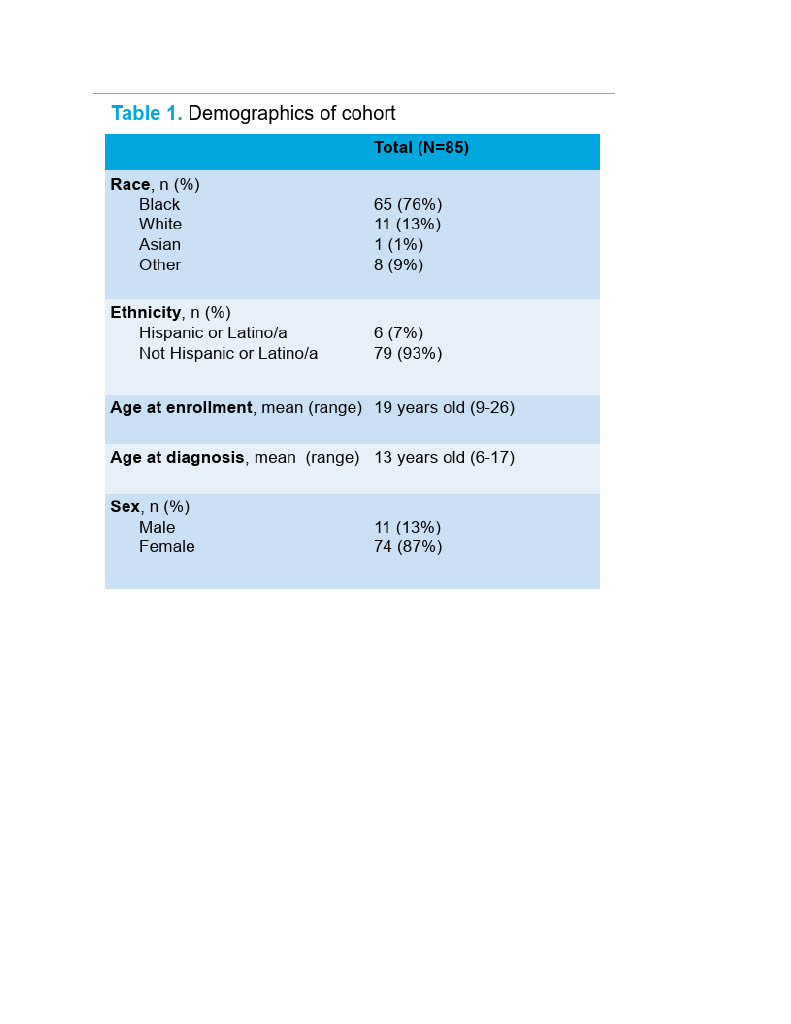 Demographics of cohort
Demographics of cohort
Table 2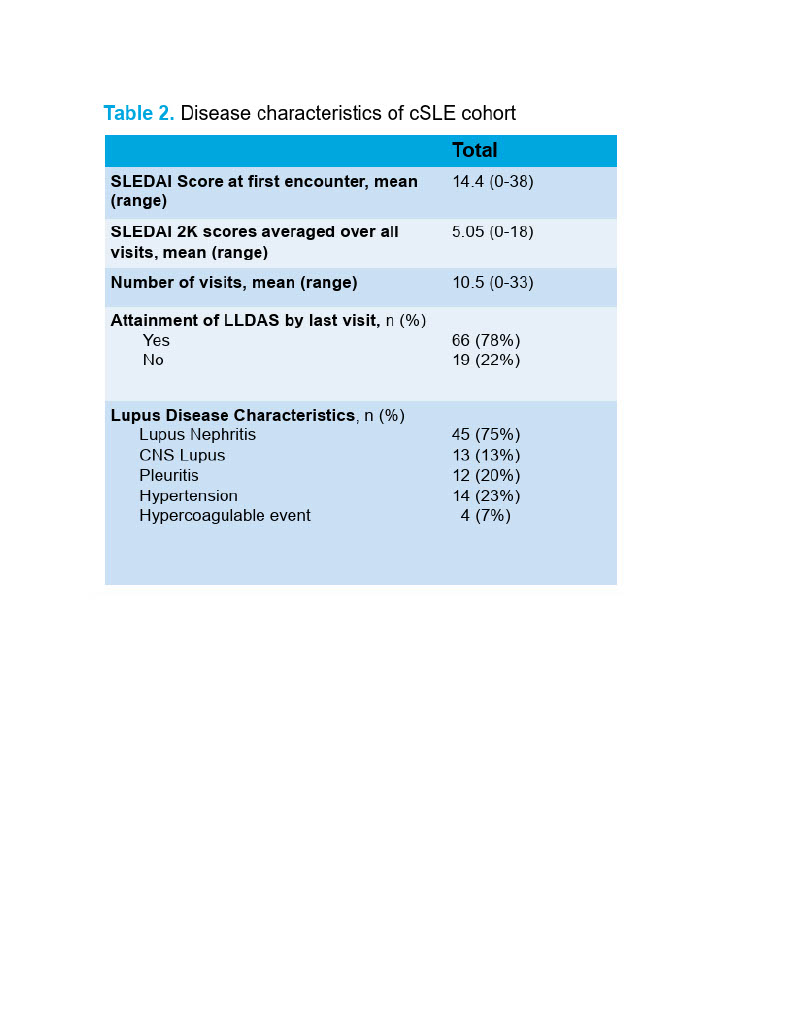 Disease characteristics of cSLE cohort
Disease characteristics of cSLE cohort
To cite this abstract in AMA style:
Reynolds C, Ruth N, Chang J. Assessing the Relationship Between Multidimensional Area Level Indicators and Lupus Disease Activity in Children [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/assessing-the-relationship-between-multidimensional-area-level-indicators-and-lupus-disease-activity-in-children-2/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/assessing-the-relationship-between-multidimensional-area-level-indicators-and-lupus-disease-activity-in-children-2/