Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose: Catastrophic antiphospholipid syndrome (CAPS) and lupus anticoagulant hypoprothrombinemia syndrome (LAHPS) represent distinct yet closely related antiphospholipid antibody-driven disease entities, caused by immune-mediated dysregulation of coagulation balance. LAHPS is a hemorrhagic disorder characterized by lupus anticoagulant (LA) positivity associated with an acquired deficiency of coagulation factor II (FII), whereas CAPS is characterized by progressive widespread microvascular thrombosis with multiorgan failure. Both entities share an underlying autoimmune etiology, with infectious or inflammatory triggers frequently unmasking their clinical phenotype. This case series contrasts two uncommon thrombotic and hemorrhagic manifestations across the shared antiphospholipid spectrum of these conditions.
Methods: With institutional review board approval, we retrospectively reviewed patients with a diagnosis of CAPS and LAHPS, from 2011 to 2024. Demographics, clinical characteristics, treatment modalities, and outcomes were collected. Descriptive statistics were utilized for analysis.
Results: We report 9 LAHPS patients (median age 11 years, 78% female, all SLE) and 7 CAPS patients (median age 13.1 years, 57% female, 43% SLE). LAHPS patients uniformly presented with hemorrhagic manifestations, including pulmonary/intracranial hemorrhage 22%, and cytopenias, including thrombocytopenia (66%) and immune hemolytic anemia (88%). Common clinical manifestations in CAPS patients included microvascular involvement of renal and neurologic systems (86%), and endocarditis (29%).
Both cohorts demonstrated high-risk antiphospholipid antibody profiles despite different clinical phenotypes. Lupus anticoagulant was detected in all LAHPS patients 100% versus 71% in CAPS; triple-positive aPL occurred in 66% of LAHPS and 43% of CAPS patients.
All patients were treated with glucocorticoids, and many received rituximab (100% LAHPS, 86% CAPS), with eculizumab used exclusively in CAPS (43%). Plasmapheresis was used in (71% of CAPS and 22% of LAHPS).
Mortality was 11% in LAHPS versus 0% in CAPS. Notably, one LAHPS patient transitioned from hemorrhagic to thrombotic phenotype during follow-up. CAPS survivors demonstrated significant morbidity, including chronic kidney disease (14%), neurologic sequelae (14%), and cardiac dysfunction (14%), while most LAHPS survivors achieved clinical remission with no recurrent episodes, with a median follow-up of 30 months.
Conclusion: LAHPS and CAPS represent life-threatening manifestations of autoimmune disease with paradoxical, severe coagulopathic presentations. Early recognition, multidisciplinary care, targeted immunomodulatory and anticoagulation therapies, and prolonged follow-up are critical, as therapeutic approaches differ substantially. Future research should focus on biomarkers to predict clinical phenotypes and guide personalized therapeutic strategies in patients with concurrent autoimmune disease and antiphospholipid antibodies.
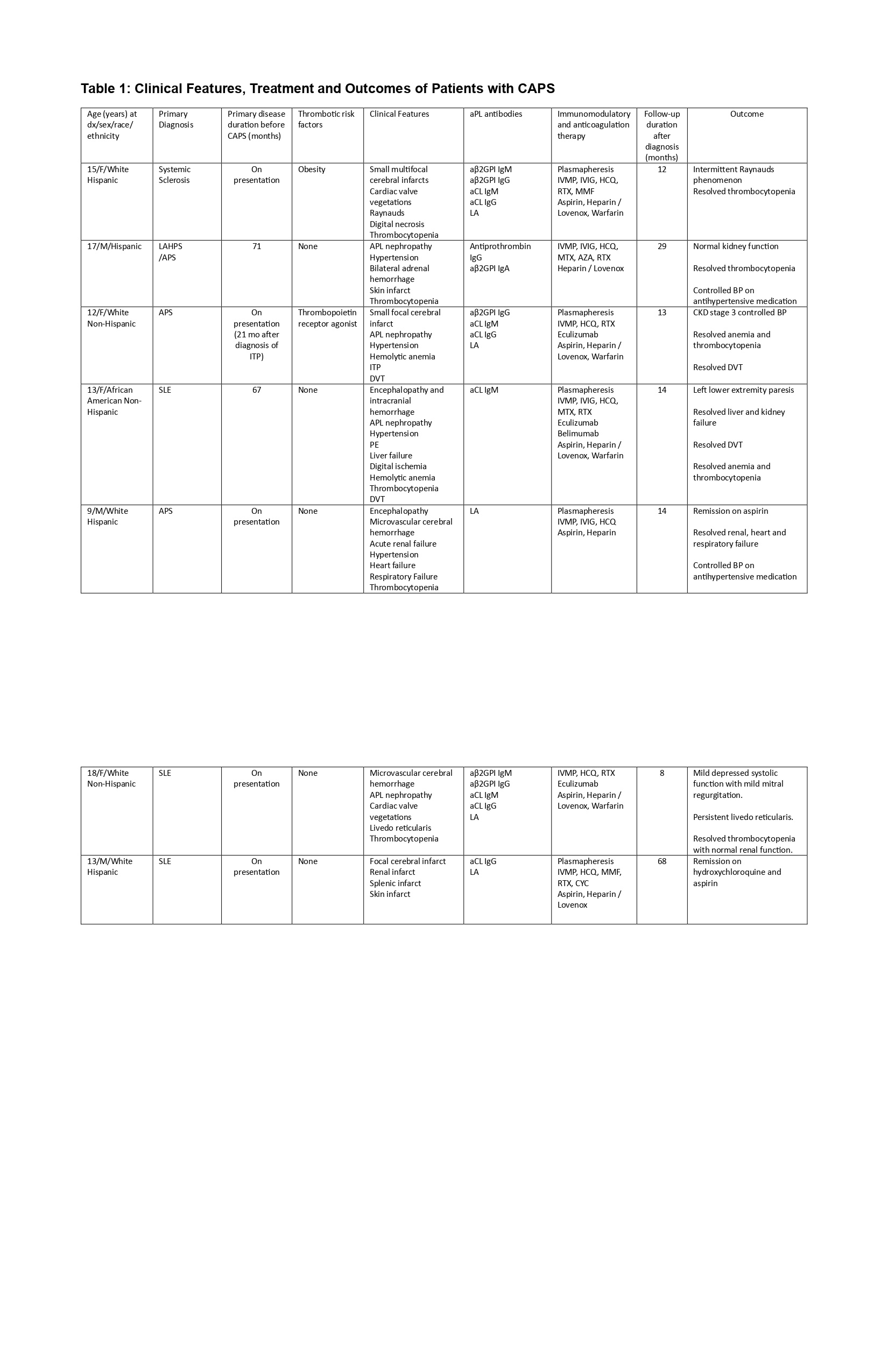 *APS = antiphospholipid syndrome; aPL = antiphospholipid; aCL = anticardiolipin; aβ2GPI = anti–β2-glycoprotein I; PE = pulmonary embolism; DVT =
*APS = antiphospholipid syndrome; aPL = antiphospholipid; aCL = anticardiolipin; aβ2GPI = anti–β2-glycoprotein I; PE = pulmonary embolism; DVT =
deep venous thrombosis; ITP = immune thrombocytopenia; LA = lupus anticoagulant; IVMP = intravenous methylprednisolone; IVIG = intravenous
immunoglobulin; RTX = rituximab; MMF = mycophenolate mofetil; AZA = azathioprine; MTX = methotrexate; CYC = cyclophosphamide; HCQ =
hydroxychloroquine; CKD = chronic kidney disease; BP blood pressure
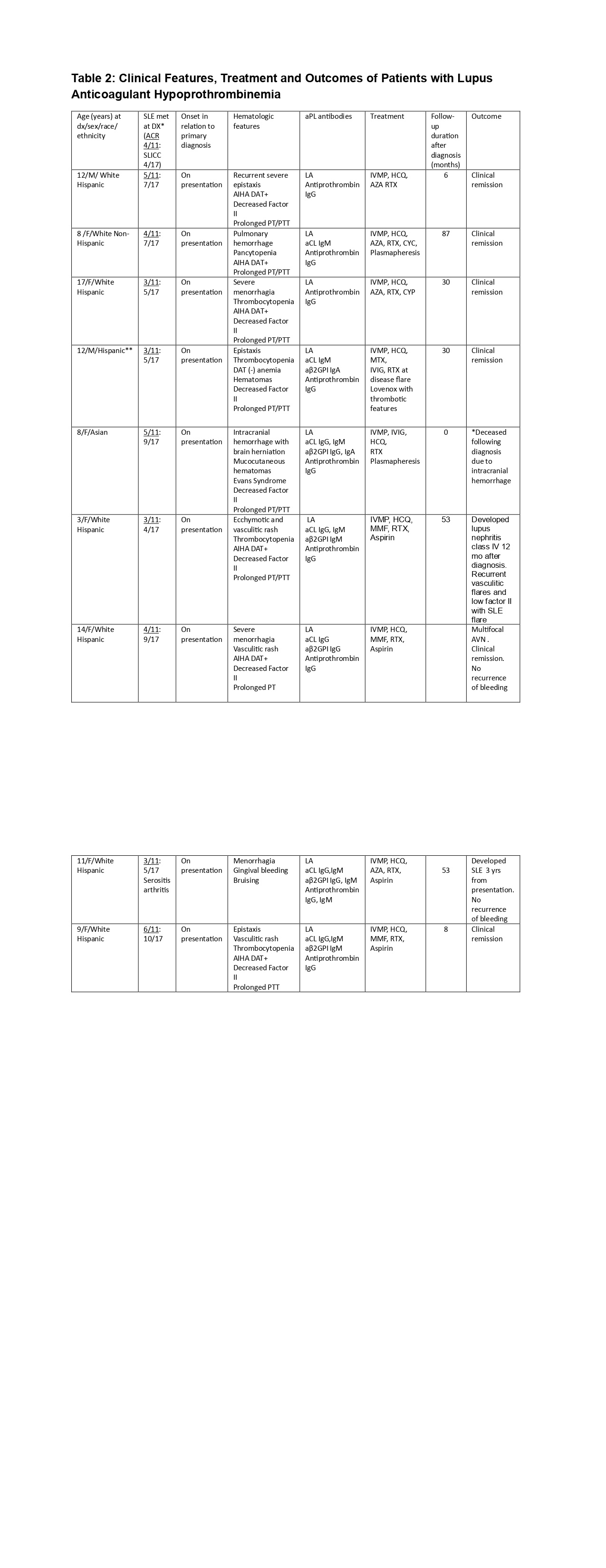 *SLE diagnosis was made according to the American College of Rheumatology (ACR) 1997 classification criteria and 2012 Systemic Lupus International Collaborating Clinics (SLICC) classification criteria
*SLE diagnosis was made according to the American College of Rheumatology (ACR) 1997 classification criteria and 2012 Systemic Lupus International Collaborating Clinics (SLICC) classification criteria
**Race not identified
***LAHPS lupus anticoagulant hypoprothrombinemia, AIHA autoimmune hemolytic anemia, DAT Direct antiglobulin test, LA lupus anticoagulant, aCL anticardiolipin; aβ2GPI anti–β2-glycoprotein I, IVMP intravenous methylprednisolone, IVIG intravenous immunoglobulin, AZA azathioprine, HCQ hydroxychloroquine, MTX methotrexate, MMF mycophenolate mofetil, RTX rituximab, CYC cyclophosphamide, AVN avascular necrosis
To cite this abstract in AMA style:
Elrefai R, Kwan O, Lai J, Pereira M, Stewart K, DeGuzman M. Antiphospholipid Antibody-Mediated Disease: Clinical Characteristics and Outcomes of Catastrophic Antiphospholipid Syndrome and Lupus Anticoagulant Hypoprothrombinemia in a Single Center Pediatric Cohort [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/antiphospholipid-antibody-mediated-disease-clinical-characteristics-and-outcomes-of-catastrophic-antiphospholipid-syndrome-and-lupus-anticoagulant-hypoprothrombinemia-in-a-single-center-pediatric-coh/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/antiphospholipid-antibody-mediated-disease-clinical-characteristics-and-outcomes-of-catastrophic-antiphospholipid-syndrome-and-lupus-anticoagulant-hypoprothrombinemia-in-a-single-center-pediatric-coh/