Session Information
Session Time: 5:23PM-5:28PM
Background/Purpose: Early childhood antibiotic exposure may impair immune development and function. Prior studies have implicated antibiotics as potential risk factors for JIA. We studied whether antibiotic exposure is associated with higher rates of new JIA diagnoses.
Methods: We conducted a nested case-control study using two large US insurance databases (public, 2001-2019; private, 2006-2023). Within a new-user cohort of children ages 0-17 years with ≥9 months of antibiotic-free time (Nf41,781,816), we identified cases with newly diagnosed JIA based on validated algorithms. Each case was matched on the JIA diagnosis (index) date to 1-10 controls with no prior JIA or immunosuppressant use by payer, year and quarter of birth and enrollment, sex, and state. We also identified cases and matched controls in a separate publicly insured cohort followed since birth (birth inception cohort, Nf35,343,408). Antibiotics were identified within the 10-months pre-index date and classified by timing, number of courses, and type. Nonbacterial antimicrobial drugs served as a negative control exposure. Associations were estimated with conditional logistic regression, adjusted for demographic, clinical, and healthcare utilization covariates, pooled across datasets via fixed-effects meta-analysis, and expressed as adjusted odds ratios (aORs) and 95% confidence intervals. Separate regression models were applied to the birth inception cohort. Secondary analyses examined subgroups (sex, age group, JIA subtype) and longer exposure periods (up to 3 years pre-index date). Sensitivity analyses examined infections and JIA in antibiotic-naïve children.
Results: A total of 5,175 cases were matched to 44,309 controls (87-88% publicly insured). Antibiotic exposure was modestly associated with new JIA in both cohorts (aOR 1.17-1.24) (Table). Stronger associations were observed with repeated antibiotic courses (new-user cohort, 1 course: aOR 1.16; 2-3 courses: aOR 1.24; 4+ courses: aOR 2.48; test for trend p< 0.001) and more recent antibiotic exposures (Figure 1). However, few differences were seen among antibiotics with differential effects on the microbiome (Figure 1). Additionally, associations for antibiotics were weaker than for non-bacterial antimicrobials (aOR 1.26-1.49) and bacterial respiratory tract, skin, and miscellaneous infections during the same periods (aOR 1.35-2.08) (Table). These same types of infections were associated with JIA in antibiotic-naïve children (aOR 1.49-3.51) (Table). Associations of antibiotics were stronger with spondyloarthritis (enthesitis-related arthritis or psoriatic arthritis) than with other JIA types (aOR 1.64-3.00) (Table, Figure 2). In contrast, antibiotic exposure was inversely associated with systemic JIA (aOR 0.56-0.64).
Conclusion: We observed dose- and time-dependent associations between antibiotic use and new JIA diagnosis. These associations may reflect preceding immune dysfunction or the role of infectious triggers in predisposed children rather than causal effects of antibiotics. However, antibiotic-related microbiome disruption may contribute to JIA development in subgroups, such as those with spondyloarthritis.
Table. Associations of antibiotics, nonbacterial antimicrobials, and infections with new JIA diagnosis. 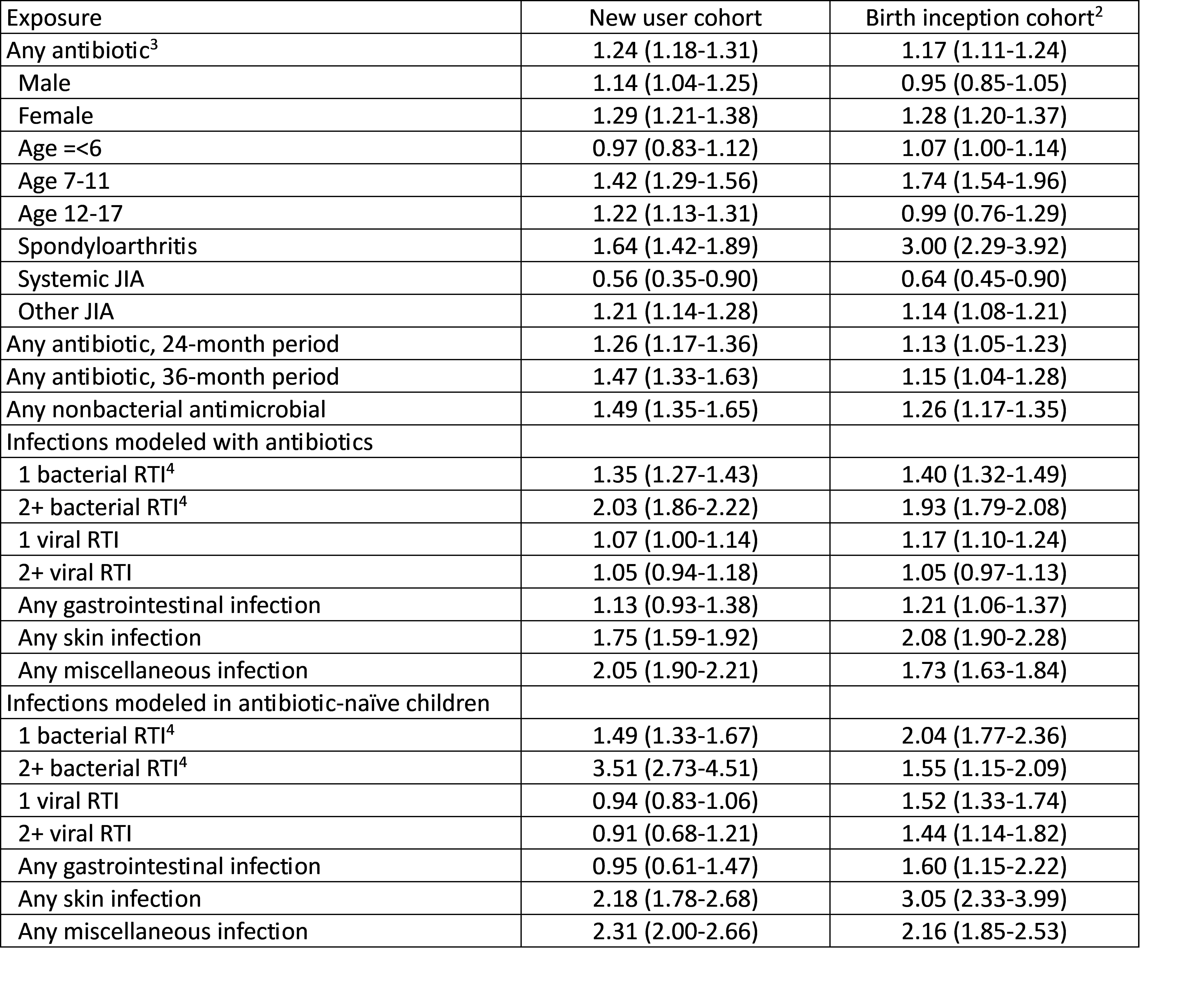 Def, definition; RTI, respiratory tract infection. 1, Conditional logistic regression models were adjusted for race, ethnicity, region, health plan type, types of infections, baseline comorbidities, and baseline healthcare utilization (outpatient visits, emergency room visit, and hospitalization), pooled across public and commercial insurance databases (except for birth inception cohort), and expressed as adjusted odds ratios (aORs) with 95% confidence intervals (CIs). 2, Publicly insured cohort followed since birth (2,137 cases, 21,293 controls). 3, 10-month exposure period, unless indicated. 4, Otitis media, sinusitis, pharyngitis, or pneumonia.
Def, definition; RTI, respiratory tract infection. 1, Conditional logistic regression models were adjusted for race, ethnicity, region, health plan type, types of infections, baseline comorbidities, and baseline healthcare utilization (outpatient visits, emergency room visit, and hospitalization), pooled across public and commercial insurance databases (except for birth inception cohort), and expressed as adjusted odds ratios (aORs) with 95% confidence intervals (CIs). 2, Publicly insured cohort followed since birth (2,137 cases, 21,293 controls). 3, 10-month exposure period, unless indicated. 4, Otitis media, sinusitis, pharyngitis, or pneumonia.
Figure 1. Associations between antibiotic exposure and new diagnosis of JIA. 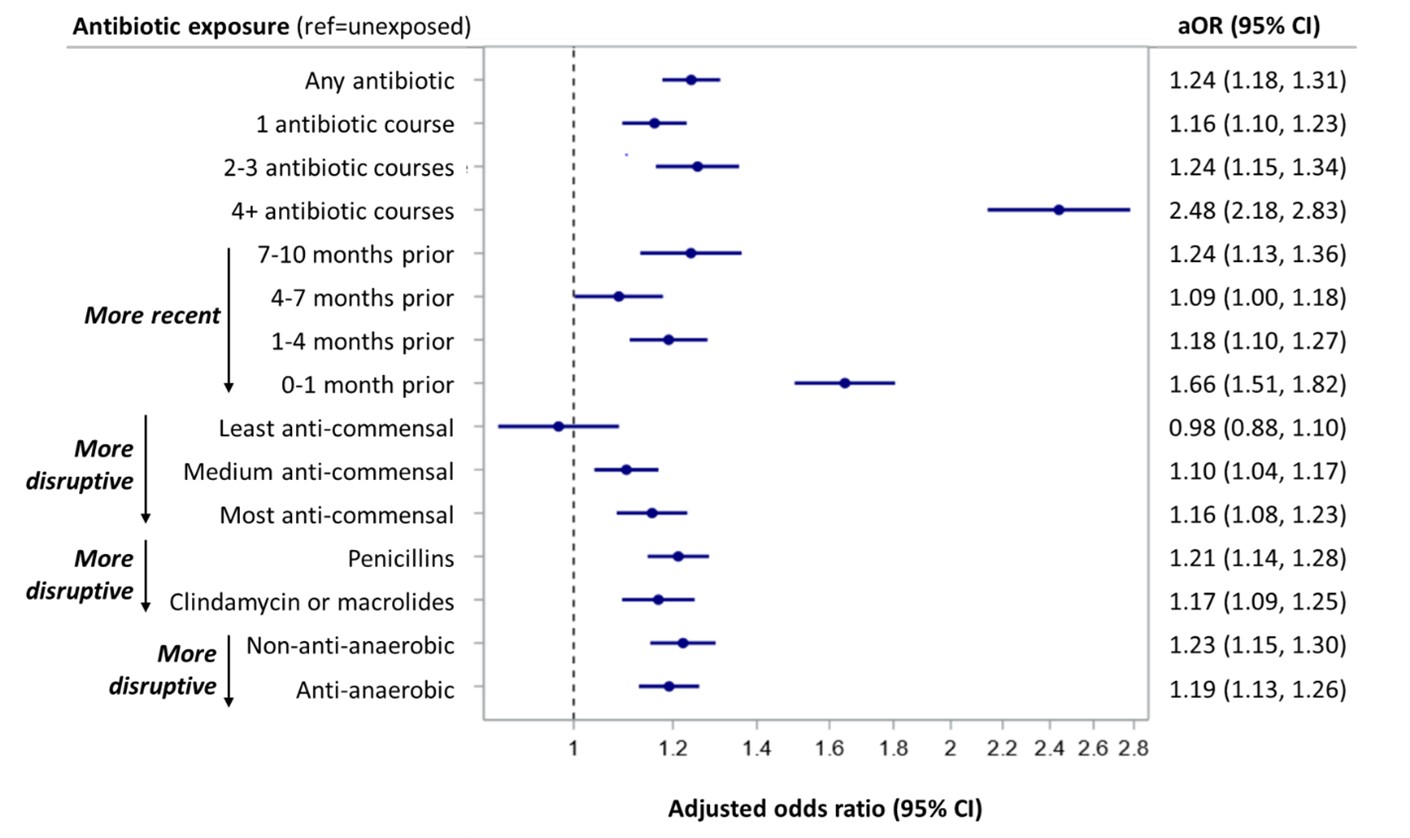 Forest plot shows associations between antibiotic exposure and new JIA diagnosis. Conditional logistic regression models were adjusted for race, ethnicity, region, health plan type, types of infections, baseline comorbidities, and baseline healthcare utilization (outpatient visits, emergency room visit, and hospitalization), pooled across public and commercial insurance databases, and expressed as adjusted odds ratios (aORs) with 95% confidence intervals (CIs).
Forest plot shows associations between antibiotic exposure and new JIA diagnosis. Conditional logistic regression models were adjusted for race, ethnicity, region, health plan type, types of infections, baseline comorbidities, and baseline healthcare utilization (outpatient visits, emergency room visit, and hospitalization), pooled across public and commercial insurance databases, and expressed as adjusted odds ratios (aORs) with 95% confidence intervals (CIs).
Figure 2. Associations between antibiotic exposure and new diagnosis of spondyloarthritis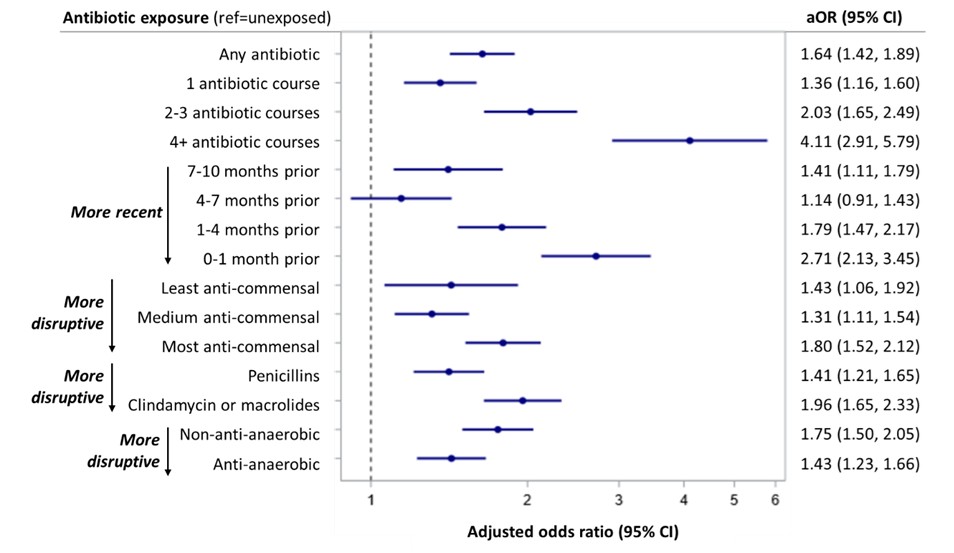 Forest plot shows associations between antibiotic exposure and new diagnosis of spondyloarthritis (enthesitis-related arthritis or psoriatic arthritis). Conditional logistic regression models were adjusted for race, ethnicity, region, comorbidities, types of infections, and healthcare utilization (outpatient visits, emergency room visit, and hospitalization), pooled across public and commercial insurance databases, and expressed as adjusted odds ratios (aORs) with 95% confidence intervals (CIs).
Forest plot shows associations between antibiotic exposure and new diagnosis of spondyloarthritis (enthesitis-related arthritis or psoriatic arthritis). Conditional logistic regression models were adjusted for race, ethnicity, region, comorbidities, types of infections, and healthcare utilization (outpatient visits, emergency room visit, and hospitalization), pooled across public and commercial insurance databases, and expressed as adjusted odds ratios (aORs) with 95% confidence intervals (CIs).
To cite this abstract in AMA style:
Rege S, Zhu Y, Parlett L, Crystal S, Davidow A, Gerhard T, Iizuka A, Iozzio M, Koffman D, Varga J, Rose C, Strom B, Horton D. Antibiotic Exposure and New Diagnosis of Juvenile Idiopathic Arthritis: A Nested Case-Control Study in a Large US Population [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/antibiotic-exposure-and-new-diagnosis-of-juvenile-idiopathic-arthritis-a-nested-case-control-study-in-a-large-us-population/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/antibiotic-exposure-and-new-diagnosis-of-juvenile-idiopathic-arthritis-a-nested-case-control-study-in-a-large-us-population/