Session Information
Date: Wednesday, October 24, 2018
Title: 6W021 ACR Abstract: Misc Rheumatic & Inflam DZ II (2970–2975)
Session Type: ACR Concurrent Abstract Session
Session Time: 11:00AM-12:30PM
Background/Purpose: The most devastating complication of Familial Mediterranean Fever is secondary AA amyloidosis and is still a problem in many cases. Efforts have been paid to prevent AA amyloidosis or to control an already formed Amyloidosis in order to prevent organ function loss, particularly renal insufficiency. There are emerging therapies in FMF related amyloidosis. Here is aimed to evaluate the role of anti-IL-1 regimens, Anakinra and Canakinumab regarding their efficacy and safety in FMF related amyloidosis.
Methods: In this single center study, 44 patients diagnosed with FMF and had a histologically proven diagnosis of amyloidosis, were exposed to anakinra or canakinumab. Patients who used anakinra less than one month and canakinumab less than 2 injections were not included in this review. For all patients recruited in this review, the indication for anti-IL-1 therapies was FMF-related amyloidosis and ongoing inflammation despite adequate colchicine treatment. Patients were questioned with regards to FMF related characteristics, comorbidities. MEFV gene status, laboratory measures, side events and therapy outcomes were tested and followed.
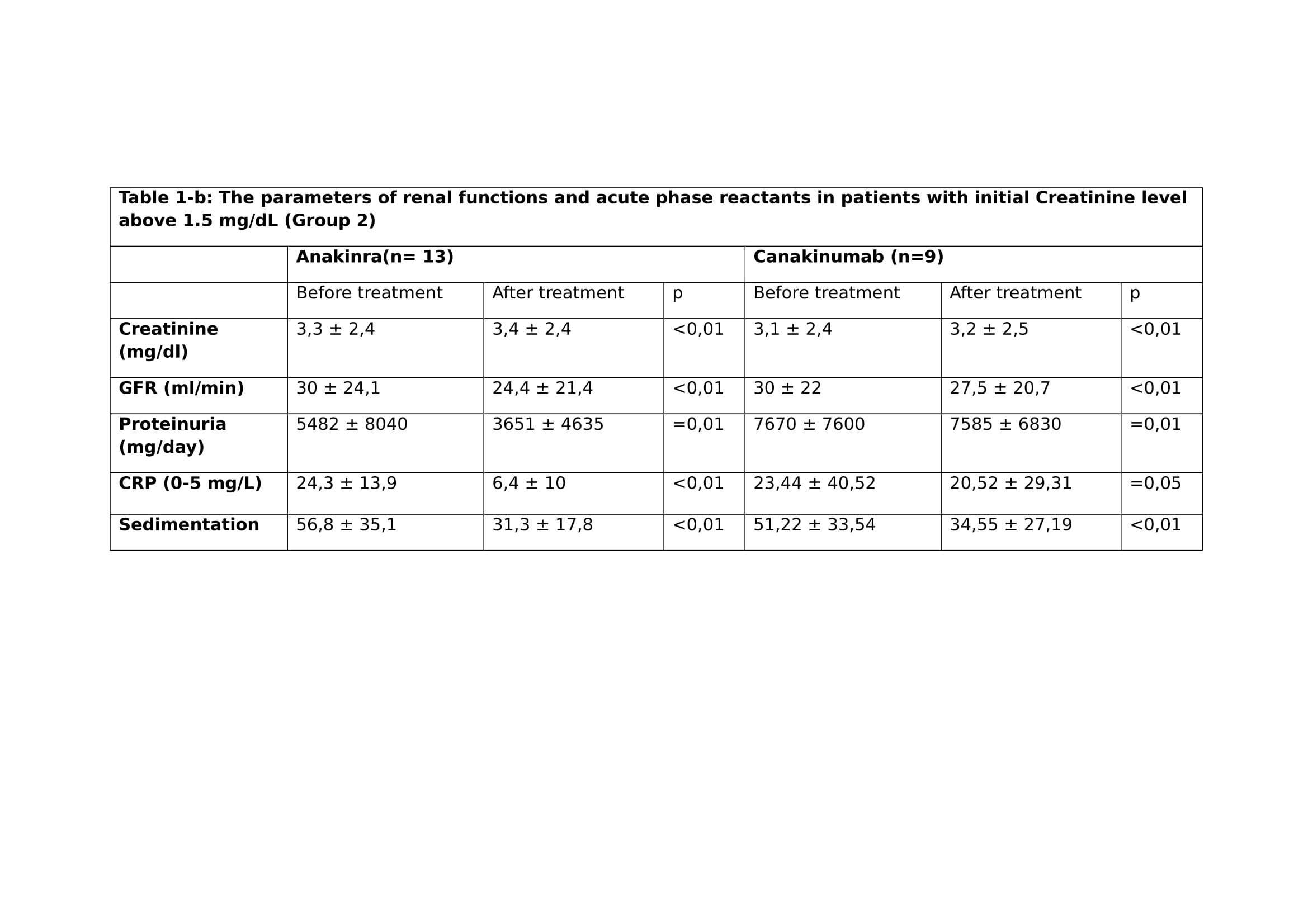
Results: Among 44 patients, 40 were initially treated with anakinra and 4 with canakinumab. Among 40 patients treated with anakinra initially, anakinra was switched to canakinumab due to allergic reactions or insufficient response in 15 patients. There are 16 patients still being treated with anakinra and 10 with canakinumab. In order to evaluate the efficacy of anti-IL-1 agents, the patients were divided into two groups with regards to their initial renal function. Patients with initial Creatinine level below 1.5 mg/dL when an anti-IL-1 drug was initiated were reviewed as Group 1 and the patients who initially had chronic renal insufficiency and Creatinine level above 1.5 mg/dL were defined as Group 2. The analysis of clinical outcome was then performed as summarized in Table 1-a and Table 1-b. The decrease in proteinuria is more modest (p=0.01) in Group 2 in comparison with Group 1 (p<0,01). At the time of this review 8 patients were still on hemodialysis. Three patients had renal transplantation.
Conclusion: In cases with FMF related AA amyloidosis, there is a need for sufficient inflammatory control. We suggest that anti-IL-1 therapies are effective and tolerable in amyloidosis. These agents are particularly effective when administered in initial stages of renal disease and the effect is less pronounced in case of an already formed renal insufficiency. The anti-IL-1 agents are generally well tolerated and the related side effects were mostly reversible.
To cite this abstract in AMA style:
Ergezen B, Ugurlu S, Selvi O, Egeli BH, Ozdogan H. Anti-Il-1 Therapies in Patients with Familial Mediterranean Fever Related AA-Amyloidosis [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/anti-il-1-therapies-in-patients-with-familial-mediterranean-fever-related-aa-amyloidosis/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/anti-il-1-therapies-in-patients-with-familial-mediterranean-fever-related-aa-amyloidosis/