Session Information
Date: Saturday, November 12, 2022
Title: Vasculitis – Non-ANCA-Associated and Related Disorders Poster I: Giant Cell Arteritis
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Giant Cell Arteritis (GCA) is the most common vasculitis in patients older than 50 years of age. GCA has significant economic burden and increases health care utilization such as Emergency Department (ED) visits and hospitalization. There is scarcity of large national level data on the reasons for presentation to the ED among patients with GCA in the United States (US). This study aims to outline the most common reasons for ED presentation among patients with GCA. We also aim to study baseline demographic characteristics, ED outcomes among patients who presented to the ED principally due to GCA.
Methods: We obtained data from the National Emergency Department Sample (NEDS) 2018 database. The NEDS is the largest publicly available ED database in the US. The NEDS is a nationally representative stratified sample of 20% of US hospital owned EDs. The 2018 NEDS contains about 35.8 million unweighted ED visits, which is roughly estimated to be about 143 million ED visits. Each ED visit in the NEDS has a principal diagnosis (the main reason for the visit) and can have up to 34 secondary diagnoses (any other diagnosis other than the principal diagnosis). We searched for ED visits for adult patients aged ≥50, with any (i.e either principal or secondary) diagnosis of GCA using ICD-10 codes “M315” or “M316”. STATA, version 16 was used for analysis. By using a “rank” command in STATA, the most common principal discharge diagnoses were divided into categories based on organ system, and the most common specific principal discharge diagnoses were recorded for ED visits among patients with any diagnosis of GCA in descending order of frequency. We then outlined baseline demographic characteristics and ED visit outcomes of patients who presented to the ED with a principal diagnosis of GCA.
Results: Out of 143 million ED visits in 2018, 20,886 (0.015%) of these visits were for patients with GCA. Rheumatologic, cardiovascular (CV), infections and respiratory were the most common reasons for presentation to the ED for patients with GCA. GCA, headaches, infectious etiologies such as sepsis, pneumonia, urinary tract infections and hypertensive heart disease with chronic kidney disease and heart failure were the most common specific principal discharge diagnosis of GCA patients who presented to the ED. See Table 1 and Figure 1Among GCA patients who presented to the ED, 3888 of these visits were principally because of GCA. ED visits principally because of GCA were predominantly elderly (mean age of 73 years), females (67.7%), admitted (59.2%), Medicare insured (77.2%), charlson comorbidity index score of less than 3 (78.4%) and presented to metropolitan teaching hospitals in the south. See Table 2.
Conclusion: GCA patients are most likely to present to the ED due to their underlying GCA. Infections and CV are also common reasons for presentation to the ED. GCA patients who presented to the ED principally due to GCA are most likely to be elderly white females and admitted. Optimizing management of GCA and its comorbidities, measures for prevention and early detection of infections while on immunosuppressants in the outpatient setting are important in preventing ED visits and hospital admissions of GCA patients.
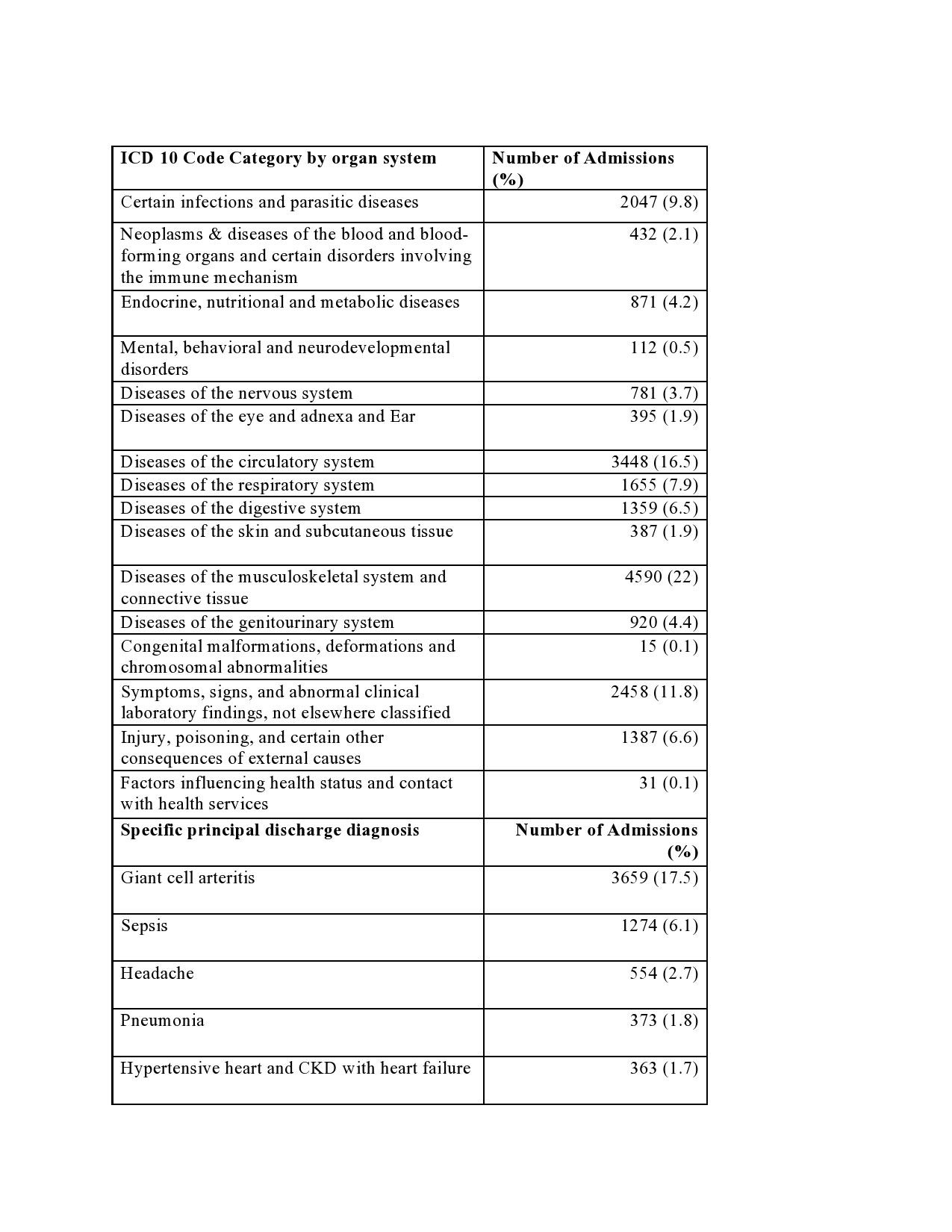
For emergency department visits of patients with any (i.e either principal or secondary) diagnosis of Giant Cell Arteritis.
COPD: Chronic obstructive pulmonary disease
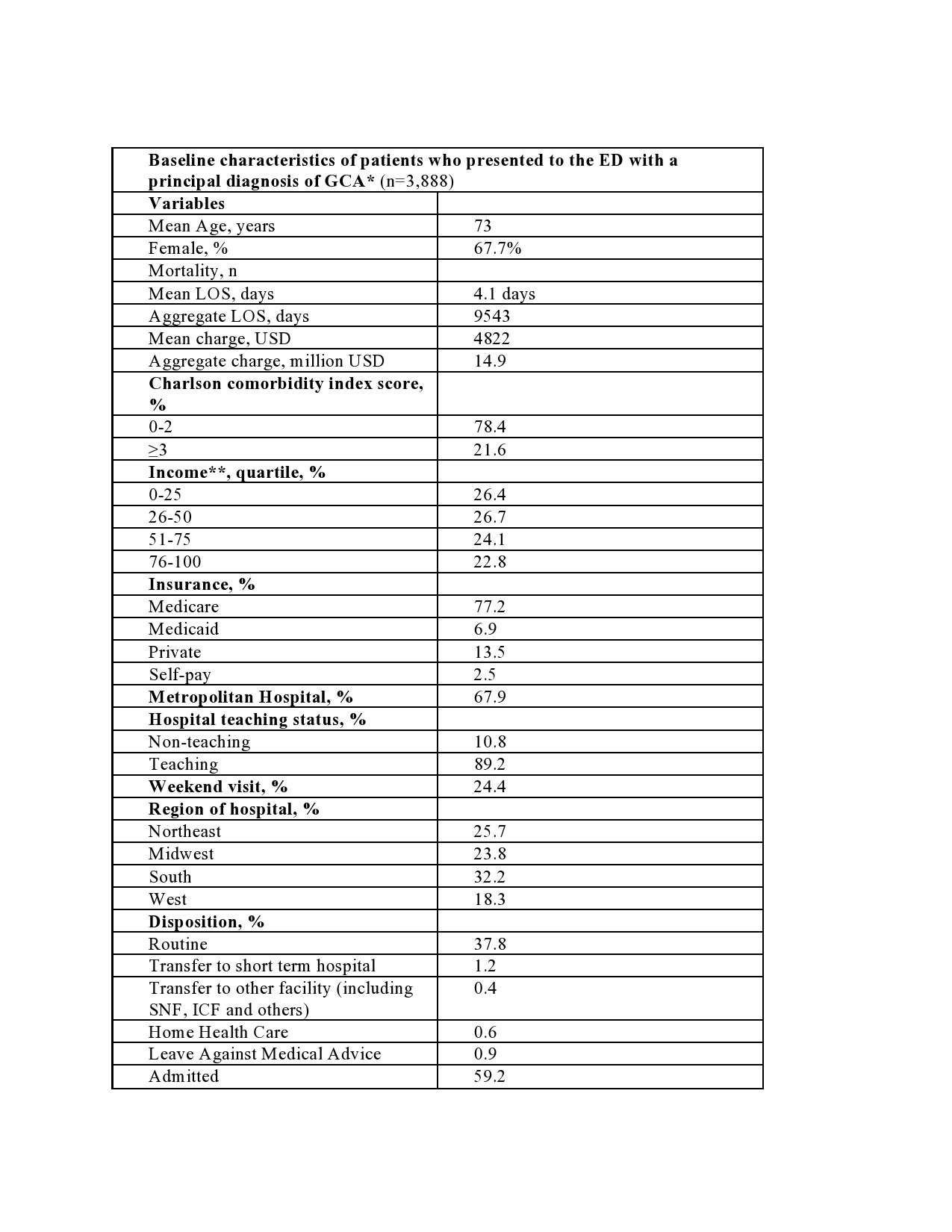
Abbreviations: * Emergency department visits for patients aged ≥ 50 years with Giant Cell Arteritis as the “principal” diagnosis, LOS: Length of inpatient stay for those admitted, Charge: charge for Emergency department visit, USD: United States dollars, income** Median household income national quartile for patient’s Zip code, SNF: Skilled nursing facility, COPD: Chronic obstruction pulmonary disease
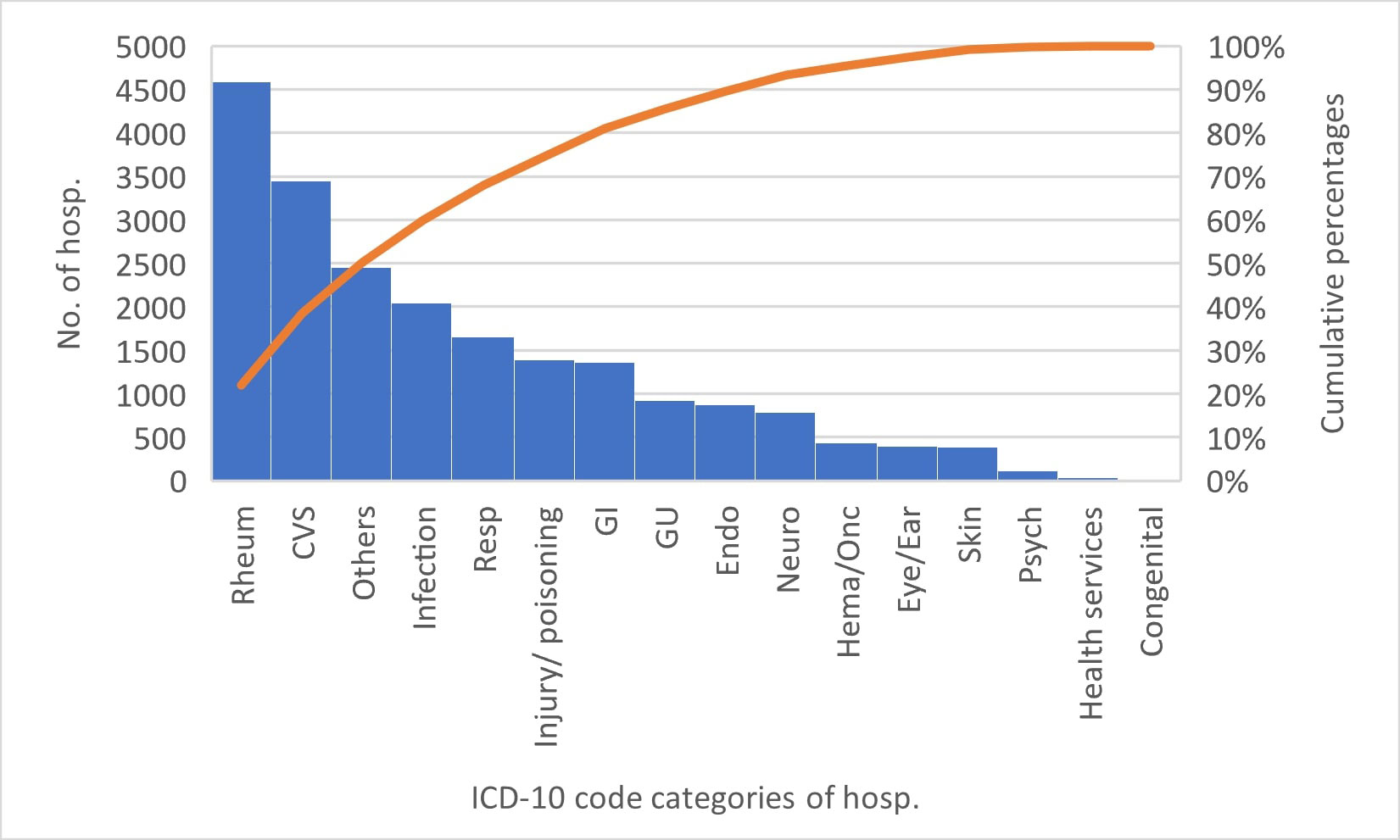
Abbreviations: Hema/Onc: Neoplasms & diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism, Endo: Endocrine, nutritional and metabolic diseases, Psych: Mental, behavioral and neurodevelopmental disorders, Neuro: Diseases of the nervous system, CVS: Diseases of the circulatory system, Respiratory: Diseases of the respiratory system, GI: Diseases of the digestive system, Rheum: Diseases of the musculoskeletal system and connective tissue, GU: Diseases of the genitourinary system, others: Symptoms, signs, and abnormal clinical laboratory findings, not elsewhere classified, Health services: Factors influencing health status and contact with health services
To cite this abstract in AMA style:
Edigin E, Trang A, Osuorji C, Anighoro S, Eseaton P, Hino C, Idolor O, Chukwu N, Akhlaq A, Hojjati M. Analysis of Emergency Department Visits by Patients with Giant Cell Arteritis: A National Population-based Study [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/analysis-of-emergency-department-visits-by-patients-with-giant-cell-arteritis-a-national-population-based-study/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/analysis-of-emergency-department-visits-by-patients-with-giant-cell-arteritis-a-national-population-based-study/