Session Information
Date: Sunday, November 12, 2023
Title: (0252–0282) Miscellaneous Rheumatic & Inflammatory Diseases Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: VEXAS syndrome (Vacuoles, E1 enzyme, X-linked, Autoinflammatory, Somatic) is a recently identified autoinflammatory disease with a large variety of disease manifestations. While recurrent fever, auricular chondritis, recurrent venous thromboembolism/thrombophlebitis, inflammatory skin lesions, ocular inflammation and cytopenias have been well-described, understanding of renal manifestations is limited.
Methods: Medical records of all patients with genetically confirmed VEXAS syndrome were reviewed for evidence of AKI or abnormal urinalysis. Patients who met the KDIGO criteria for acute kidney injury (AKI) for at least two consecutive measurements of serum creatinine or cystatin C were considered as having AKI. Biopsy specimens (n = 4) were reviewed by four experienced nephropathologists. Clinical and laboratory features at disease onset and at time of AKI diagnosis were abstracted from direct chart review.
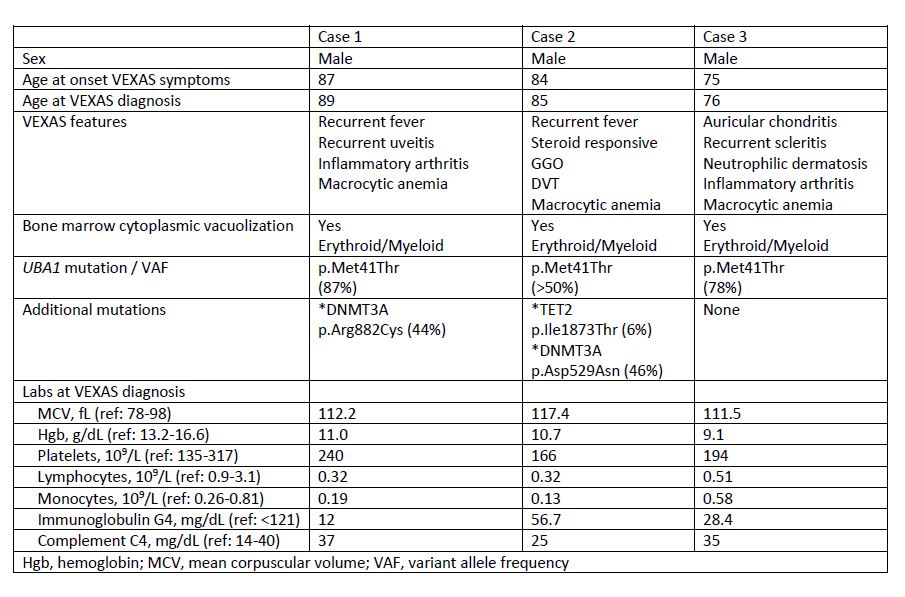
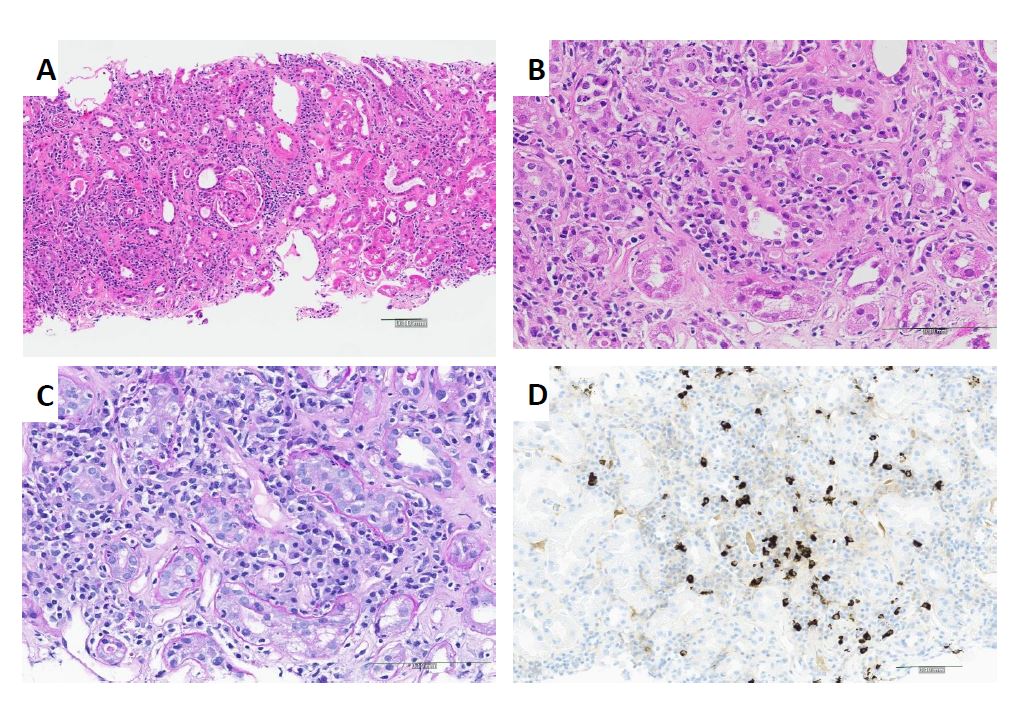
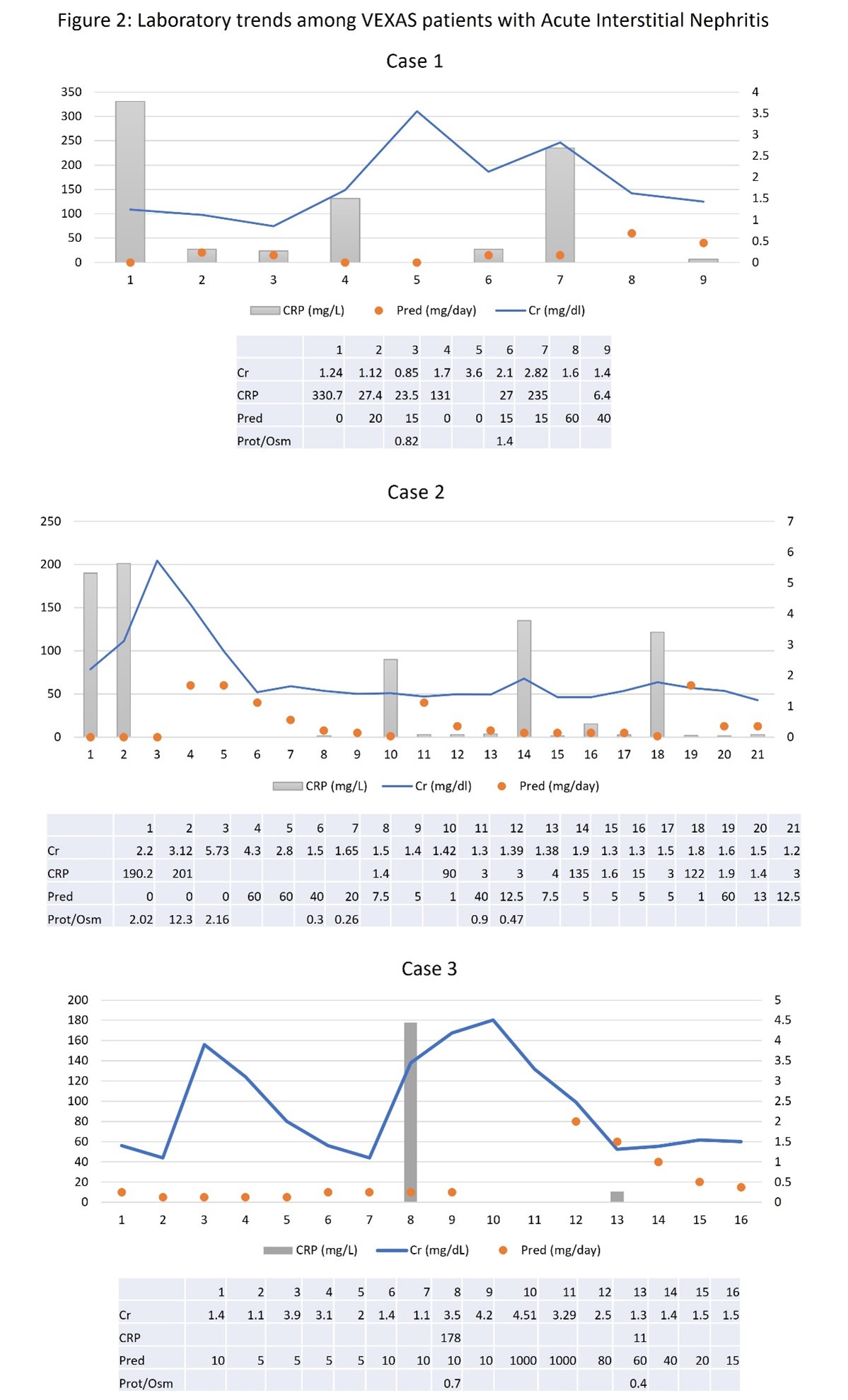
Results: Among a cohort of 69 patients (all men, mean age 71 ± 9) with VEXAS syndrome, 16 (23%) developed AKI (mean age 75 ± 9) at some point during their follow up. A review of urinary findings among patients with AKI revealed microscopic hematuria, mild proteinuria, and pyuria in 100%, 100% and in 82% of cases, respectively. Four patients had undergone renal biopsy for acute kidney injury. One patient had features of peri-tubular capillaritis and has been previously described. Three patients were found to have biopsy confirmation of IN. Clinical features are described in Table 1. A representative biopsy is shown in Figure 1. All three patients had IN (acute in 2 and active chronic in 1) with plasma cell-rich infiltrate and tubulitis. Two patients had focal increased numbers of IgG4 staining cells (one 30/hpf, one 17/hpf) but the IgG4:IgG was low and no other pathologic features suggestive of IgG4-related disease were seen. None of the patients had clinical or radiographic features of IgG4-RD and all had normal serum IgG4 values. Arteritis, granulomatous inflammation and glomerulonephritis were absent. Immunofluorescence was negative and electron microscopy did not show glomerular or extraglomerular immune deposits. Protein/osmolality ratio was increased at the time of active systemic inflammation and renal compromise. Prednisone was initiated in all patients with biochemical improvement in renal function (Figure 2), however, subsequent decline in renal function corresponded with reduction in prednisone dose below 10-15 mg/day. All three patients carried the p.Met41Thr mutation and two patients had additional clonal hematopoietic mutations (DNMT3A, TET2).
Conclusion: AKI from Plasma cell-rich IN is an under-recognized feature in patients with VEXAS. Physicians should be aware of this complication, which should be considered in patients with VEXAS and acute kidney injury. Prompt treatment with high-dose glucocorticoids can result in improvement of renal function. Further study regarding laboratory and urinary parameters that identify active versus inactive renal disease are needed. Identification of targeted, effective therapy is necessary.
To cite this abstract in AMA style:
Koster M, HerreraHernandez L, Bu L, Montes D, Nasr S, Cornell L, Warrington K, Patnaik M, Mangaonkar A, Kalantari K. Acute Kidney Injury and Plasma Cell-Rich Acute Interstitial Nephritis in VEXAS Syndrome: An Under-recognized Disease Feature [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/acute-kidney-injury-and-plasma-cell-rich-acute-interstitial-nephritis-in-vexas-syndrome-an-under-recognized-disease-feature/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/acute-kidney-injury-and-plasma-cell-rich-acute-interstitial-nephritis-in-vexas-syndrome-an-under-recognized-disease-feature/