Session Information
Date: Monday, November 9, 2015
Title: Rheumatoid Arthritis-Small Molecules, Biologics and Gene Therapy IV: Safety of Targeted Therapies
Session Type: ACR Concurrent Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose:
Tofacitinib is an oral
Janus kinase inhibitor for the treatment of rheumatoid arthritis (RA). In Phase
3 (P3) studies, tofacitinib demonstrated safety and efficacy at 5 and 10
mg BID when used as monotherapy or with conventional synthetic (cs) DMARDs
(csDMARDs). Here, we examine the safety profile of tofacitinib 5 mg BID as
monotherapy and combination therapy in the P3 RA program.
Methods: Safety data for tofacitinib were obtained
from six double-blind P3 studies of 6–24 months duration and stratified by
whether tofacitinib was administered as monotherapy (NCT00814307, ORAL Solo; NCT01039688,
ORAL Start) or with csDMARDs (NCT00960440, ORAL Step; NCT00847613, ORAL Scan; NCT00856544,
ORAL Sync; and NCT00853385, ORAL Standard). Patients (pts) in ORAL Start were methotrexate
(MTX)-naïve while pts in all other studies had an inadequate response to cs or
biologic DMARDs. Endpoints included:
serious adverse events (SAEs),
discontinuations due to adverse events (AEs), serious infection events (SIEs), opportunistic
infections, herpes zoster (HZ), malignancies, major adverse cardiovascular
events, gastrointestinal perforations, all-cause mortality, and laboratory
safety data.
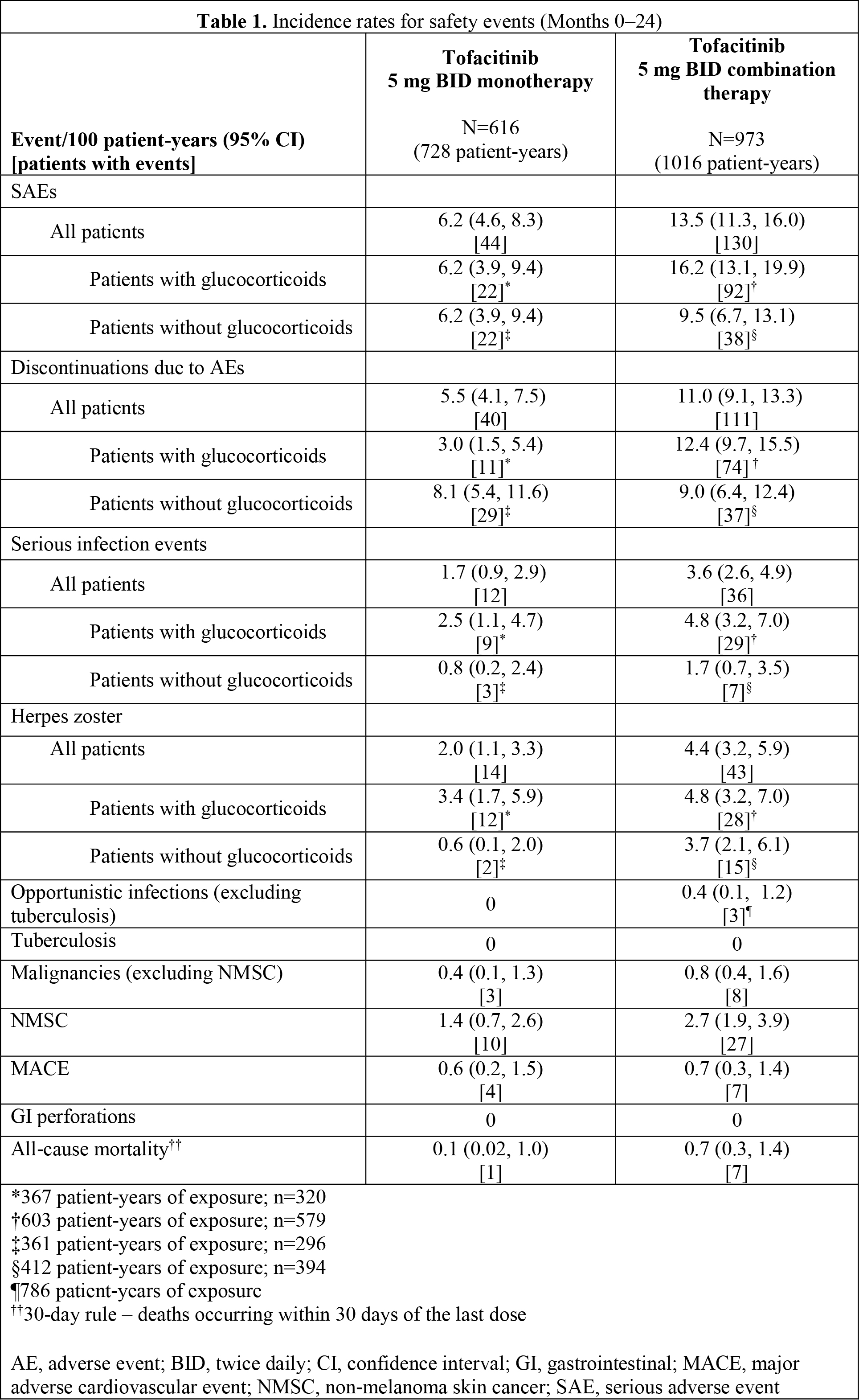
Results: Tofacitinib 5 mg BID was administered as
monotherapy in 616 pts (243 from ORAL Solo and 373 from ORAL Start, mean
age 51.1 years [yrs], mean RA duration 4.9 yrs, 49.8% received glucocorticoids
[GC]) and combination therapy in 973 pts (mean age 53.4 yrs, mean RA duration
8.9 yrs, 57.8% received GC). Incidence rates (IRs) for SAEs, discontinuations
due to AEs, SIEs and HZ were generally lower in pts receiving tofacitinib monotherapy
vs combination therapy. A similar trend was observed when pts were stratified
by GC use; however confidence intervals were wide and overlapping for some
outcomes (Table 1). IRs for SIEs and HZ were greater for pts who received GC compared
with those who did not irrespective of whether tofacitinib was given as
monotherapy or in combination. Similar proportions of pts in the monotherapy
and combination therapy groups had confirmed laboratory decreases in
hemoglobin, neutrophil and lymphocyte counts, and increases in liver enzymes
and serum creatinine (Table 2).
Conclusion: In this analysis, IRs for SAEs, discontinuations due
to AEs, SIEs, and HZ were lower in the tofacitinib 5 mg BID monotherapy group
vs the combination therapy group; however, IRs should be interpreted with
caution as the data are from controlled studies of limited duration and
MTX-naïve pts with shorter disease duration were included in the monotherapy
group only.

To cite this abstract in AMA style:
Kivitz AJ, Haraoui B, Kaine J, Castellano V, Bananis E, Connell CA, Hoffman E, Takiya L. A Safety Analysis of Tofacitinib 5mg Twice Daily Administered As Monotherapy or in Combination with Background Conventional Synthetic Dmards in a Phase 3 Rheumatoid Arthritis Population [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/a-safety-analysis-of-tofacitinib-5mg-twice-daily-administered-as-monotherapy-or-in-combination-with-background-conventional-synthetic-dmards-in-a-phase-3-rheumatoid-arthritis-population/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-safety-analysis-of-tofacitinib-5mg-twice-daily-administered-as-monotherapy-or-in-combination-with-background-conventional-synthetic-dmards-in-a-phase-3-rheumatoid-arthritis-population/