Session Information
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Periodic fever syndromes (PFS) is a group of rare autoinflammatory diseases that includes cryopyrin-associated periodic syndromes (CAPS), hyperimmunoglobulin D syndrome/mevalonate kinase deficiency (HIDS/MKD), TNF receptor-associated periodic syndrome (TRAPS), and familial Mediterranean fever (FMF). Although canakinumab (CAN) has been approved in the United States (US) for patients (pts) with the aforementioned PFS, there have been limited studies on prescribing patterns among physicians who have initiated CAN in real world settings. We assessed the clinical and treatment profiles of PFS pts who were prescribed CAN and the physician reason(s) for initiating CAN in US clinical practice.
Methods: Online medical charts were reviewed retrospectively to collect data from US rheumatologists/ dermatologists/ allergists / immunologists on pts (pediatrics [Ped; < 18 yrs] and adults [Adt; ≥18 yrs]) diagnosed with PFS who were initiated on CAN therapy by the responding physician between 2016 and 2018. Online case report forms were used to collect information on pt demographics, disease characteristics at CAN initiation, pre-CAN treatment history, and CAN prescribing patterns. Reasons for discontinuation of previous treatment and initiation of CAN were also collected.
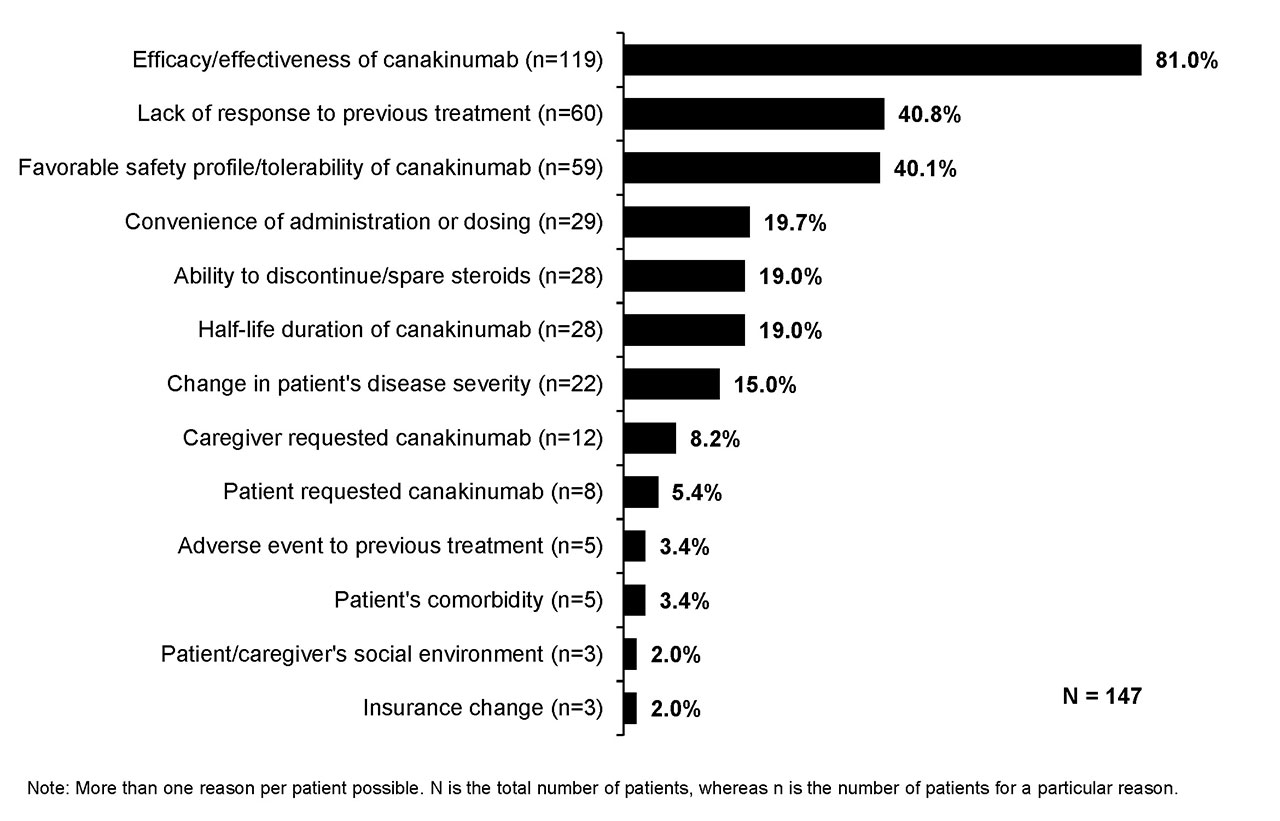
Results: Medical charts were reviewed by 58 physicians who had specialty in rheumatology (26; Adt 88%, Ped 12%), dermatology (15; Adt 73%, Ped 27%), allergy (9; Adt 44%, Ped 56%), and immunology (8; Adt 38%, Ped 62%). Of the 147 pts, 57% were male and 46% were Ped. The mean age at CAN initiation was 21.7 yrs (Adt, 31.9 yrs; Ped, 9.9 yrs). Among PFS subtypes, 37% pts had CAPS, 27% TRAPS, 27% FMF, 7% HIDS/MKD and 3% mixed PFS subtypes. Median age at PFS diagnosis was 13 yrs (IQR: 6-20 yrs). The key methods of diagnosis were assessment of clinical symptoms and complications (87%), age of onset (63%), and family history/ancestry (57%). The main diagnoses which were ruled out included fever of unknown origin (70%), urticaria or rash/allergy (54%), and recurrent infection (51%). The severity of PFS was mild (22%), moderate (69%), or severe (8%) at CAN initiation. The most common symptoms at CAN initiation were fever (79%), fatigue/malaise (57%), skin rashes (44%), erythema (29%), arthralgia (26%), and myalgia (25%). Most pts (91%) received other long-term treatments in the last line of therapy prior to CAN including NSAIDs (28%), anakinra (24%), and colchicine (22%). The main reasons for discontinuation of treatment prior to CAN were lack of efficacy/effectiveness (40%) and availability of a new treatment (36%; Fig. 1). Decision to start CAN was made by both physician and pt/caregiver (61%), by physician only (35%), and by pt/caregiver only (4%). The prime reasons for CAN initiation included efficacy/effectiveness (81%), lack of response to previous treatment (41%) and favorable safety/tolerability profile (40%; Fig. 2).
Conclusion: Results from this study provide insight into the reasons for CAN initiation in PFS pts, with efficacy/effectiveness, lack of response to previous treatment and favorable safety/tolerability profile being the most common reasons.

To cite this abstract in AMA style:
Hur P, Lomax K, Ionescu-Ittu R, Manceur A, Xie J, Cammarota J, Sanghera N, Grom A. A Retrospective Medical Chart Review of Patients with Periodic Fever Syndromes Initiating Canakinumab in the United States [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/a-retrospective-medical-chart-review-of-patients-with-periodic-fever-syndromes-initiating-canakinumab-in-the-united-states/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-retrospective-medical-chart-review-of-patients-with-periodic-fever-syndromes-initiating-canakinumab-in-the-united-states/