Session Information
Date: Sunday, November 12, 2023
Title: (0252–0282) Miscellaneous Rheumatic & Inflammatory Diseases Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Idiopathic Granulomatous Mastitis (IGM) is a rare often self-limited chronic inflammatory breast disease of unknown etiology characterized by non-caseating granulomas in breast tissue, affecting primarily women of child-bearing age. The diagnosis is made by histological examination after excluding other conditions (particularly malignancy and infections).Management options are limited and include observation, antibiotics, corticosteroids, and methotrexate (MTX). Progression and recurrence are common despite treatment. We present a series of patients referred to a rheumatology practice.
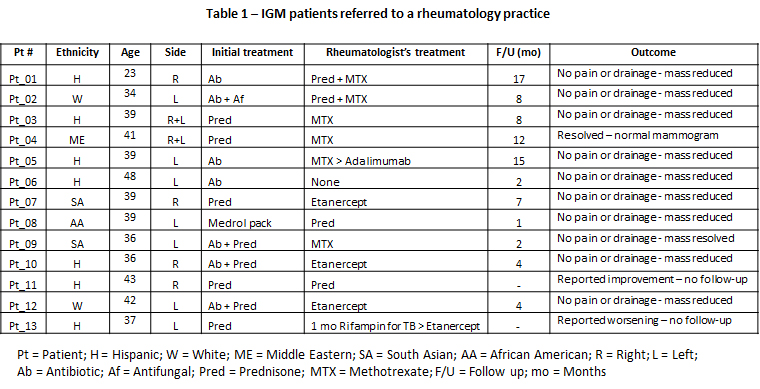
Methods: We reviewed the charts of all patients referred to a rheumatology practice with biopsy-confirmed diagnosis of IGM (2019-2023). Demographics, clinical information, and treatment are summarized in Table 1. For the purpose of this report, we defined improvement as the patients’ subjective assessment of their pain/discomfort; the disappearance of discharge; and a reduction/disappearance of the breast mass(es).
Results: Thirteen parous women (median age 39 yrs, range 23 – 48) were referred to us by a breast surgery practice to exclude possible causes for their granulomatous breast masses. Biopsy revealed non-necrotizing granulomas and no malignancy; cultures were negative for bacteria, mycobacteria, and fungi. All patients were otherwise in good health. We obtained ANCA panel, ACE levels, and chest X-ray to gain insights into possible non-caseating granulomatous diseases (e.g., sarcoidosis and ANCA-associated vasculitis). All test results were normal. Previous treatments by the referring breast surgeon, including antibiotics or anti-fungal only (4 patients), antibiotics and corticosteroids (3 patients), and corticosteroids only (6 patients), had failed to induce improvement (as defined above). Only one patient (#6 in table 1) improved with antibiotics alone (after referral) and did not require follow-up; two patients (#8 and #11) improved with continuing corticosteroids; MTX was used in 6 patients, alone (#3. #4, #9), as steroid sparing (#1, #2), or in association with an anti-TNF-α (#5). In 5 patients with persistent or recurrent manifestations (multiple masses, marked drainage, severe pain) we added anti-TNF-α agents (etanercept or adalimumab). Four of the 5 patients (#5, #7, #10, and #12) experienced substantial clinical improvement and the lesions resolved completely (in one case confirmed by mammogram). Patient #13 reported worsening of her symptoms after one dose of etanercept and refused to return for a follow-up appointment.
Conclusion: There are no evidence-based guidelines on the management for IGM. Treatments include observation, antibiotics, systemic or intra-lesional corticosteroids, MTX (alone or as steroid sparing), and rarely surgery. Many patients do not tolerate systemic corticosteroids; MTX is contraindicated in child-bearing women without contraception. Anti-TNF-α agents may represent a safer treatment. The rationale for their use is that by blocking TNF-α, a cytokine that plays a major role in forming and maintaining granulomas, these agents may provide an effective and targeted alternative, making rheumatologists pivotal partners in the management of IGM.
To cite this abstract in AMA style:
Genta M, DiPasquale A. A Novel Role for Rheumatologists: Managing Idiopathic Granulomatous Mastitis [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/a-novel-role-for-rheumatologists-managing-idiopathic-granulomatous-mastitis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-novel-role-for-rheumatologists-managing-idiopathic-granulomatous-mastitis/