Session Information
Session Type: Poster Session (Sunday)
Session Time: 9:00AM-11:00AM
Background/Purpose: PMR is associated with a pattern of abnormal 18F-Fluorodeoxyglucose (18F-FDG) uptake on whole body PET/CT that is increasingly recognised to correlate anatomically with inflammation of extracapsular structures.(1) The aim of this study was to evaluate the sensitivity and specificity of PET/CT findings in PMR including novel involvement at the posteromedial knee and develop a representative diagnostic scoring algorithm utilising results from a minimum number of musculoskeletal sites.
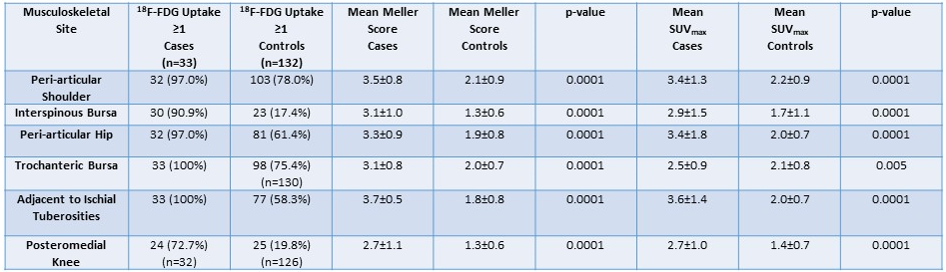
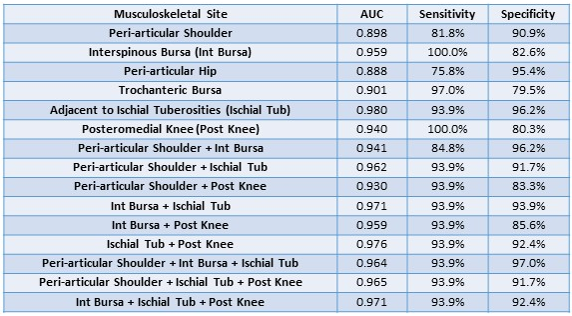
Methods: Steroid-naïve patients with newly diagnosed PMR (2012 EULAR/ACR classification criteria) were prospectively recruited. Participants with giant cell arteritis were excluded. A whole body 18F-FDG PET/CT scan from skull vertex to toes was performed at baseline. Each PMR case was age- and sex-matched to four consecutive historic PET/CT controls, with relevant data pertaining to scan indication, underlying diagnosis and medical history extracted from the clinical record. Qualitative (Meller score) and semi-quantitative scoring (standardised uptake value maximum [SUVmax]) of abnormal 18F-FDG uptake at 21 musculoskeletal sites was undertaken for cases and controls. Results were compared using the Mann-Whitney U test, a p-value < 0.05 being considered statistically significant. Receiver operating characteristics (ROC) curves were generated for abnormal findings at each musculoskeletal site, along with calculation of the area under the curve (AUC), sensitivity and specificity.
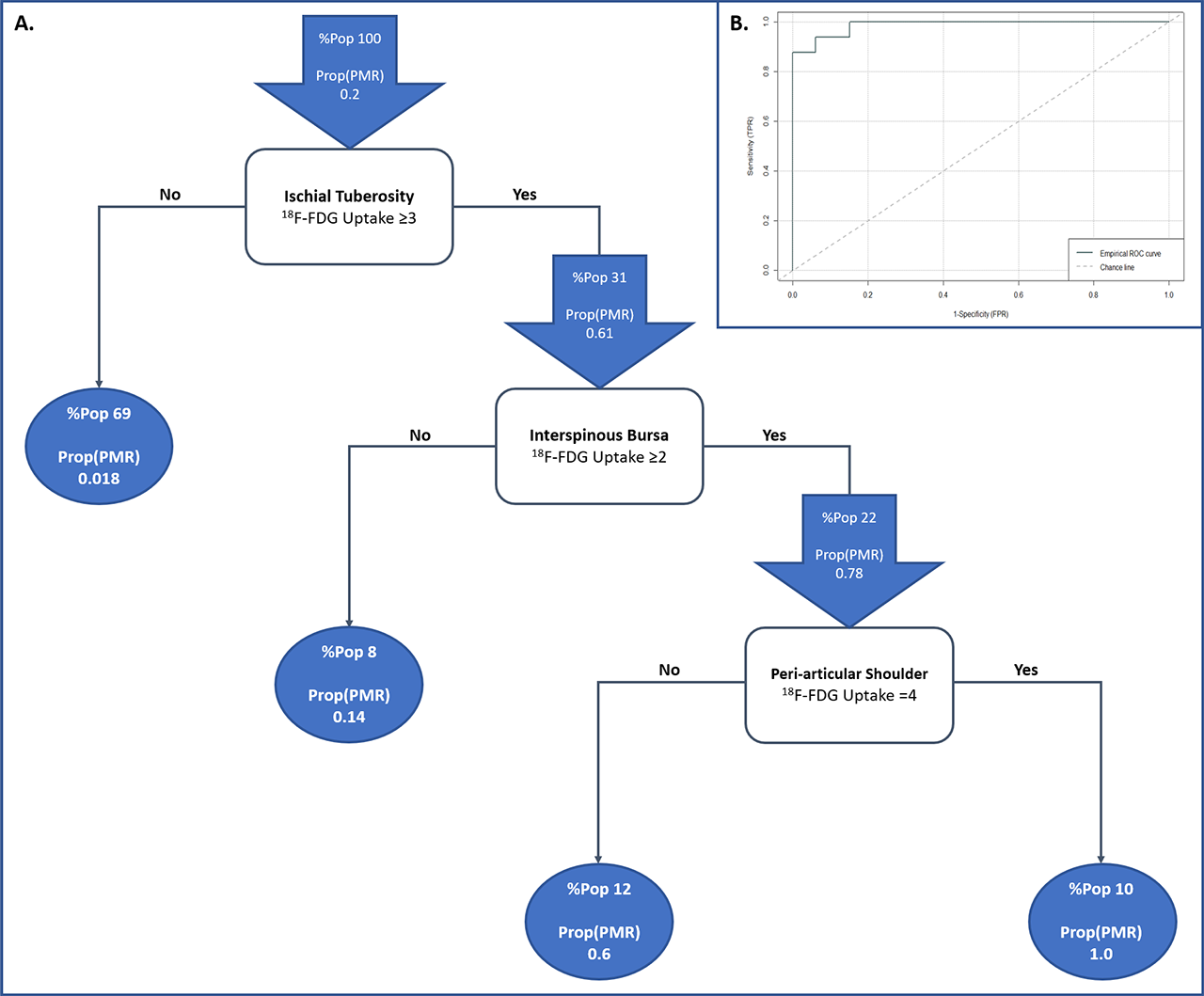
Results: 33 cases met the inclusion criteria and were matched to 132 controls. Mean age was 68.6±7.4 years for cases cf. 68.2±7.3 for controls, and 54.5% of patients were male. Mean EULAR/ACR score was 5.2±0.6 for the PMR group, with median CRP 49 (32 – 65) and ESR 41.5 (24.6 – 64.4). The predominant indication for whole body PET/CT in the controls was malignancy (47.0%). 43/132 controls (32.6%) had a history of a rheumatic condition including 9 (6.8%) with an inflammatory arthritis. Table 1 summarizes the incidence of abnormal findings on whole body PET/CT in cases compared with controls. Individual musculoskeletal sites proved insufficient for diagnostic purposes, however 18F-FDG uptake at the peri-articular shoulder in combination with interspinous bursa and adjacent to the ischial tuberosities achieved a sensitivity of 93.9% and specificity of 97% (Table 2). A diagnostic algorithm utilising scores at each of these 3 musculoskeletal sites is depicted in Figure 1 (AUC 0.987; sensitivity 93.9%, specificity 93.9%). When tested on the study population, none of the controls were misdiagnosed with PMR.
Conclusion: The combination of abnormal 18F-FDG uptake at the peri-articular shoulder, interspinous bursa and adjacent to the ischial tuberosities on whole body PET/CT is highly sensitive and specific for a diagnosis of PMR.
(1) Owen CE, Poon AMT, Lee ST, Yap LP, Zwar RB, McMenamin CM, et al. Fusion of positron emission tomography/computed tomography with magnetic resonance imaging reveals hamstring peritendonitis in polymyalgia rheumatica. Rheumatology. 2018;57(2):345-53.
To cite this abstract in AMA style:
Owen C, Poon A, Yang V, McMaster C, Lee S, Liew D, Leung J, Scott A, Buchanan R. A Novel Diagnostic Algorithm for Polymyalgia Rheumatica Using Three Musculoskeletal Sites on Whole Body PET/CT [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/a-novel-diagnostic-algorithm-for-polymyalgia-rheumatica-using-three-musculoskeletal-sites-on-whole-body-pet-ct/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-novel-diagnostic-algorithm-for-polymyalgia-rheumatica-using-three-musculoskeletal-sites-on-whole-body-pet-ct/