Session Information
Session Type: Late-Breaking Abstract Session
Session Time: 4:00PM-6:00PM
Background/Purpose: Telitacicept, also named RC18, is a novel recombinant fusion protein constructed with the extracellular domain of the human transmembrane activator and calcium modulator and cyclophylin ligand interactor (TACI) receptor and the Fc domain of human immunoglobulin (Ig) G1 targeting and neutralizing B lymphocyte stimulator (BLyS) and a proliferating-inducing ligand (APRIL). This phase 2b study evaluated the efficacy and safety of Telitacicept versus placebo in combination with standard therapy in SLE patients.
Methods: SLE patients aged 18 to 65 years with positive ANA and/or anti-dsDNA and with a SELENA-SLEDAI score ≥8 were randomized 1:1:1:1 to receive subcutaneous Telitacicept at 80 mg, 160 mg, 240 mg or placebo once a week in combination with standard therapy for 48 weeks. The primary endpoint was response rate of SLE Responder Index 4 (SRI4) at Week 48. The SRI4 response was defined as: ≥4 points reduction from baseline in SELENA-SLEDAI score, and no new BILAG A organ domain score or 1 new BILAG B organ domain score compared with baseline, and no worsening (increase of < 0.30 points from baseline) in Physician’s Global Assessment (PGA). This trial is registered with ClinicalTrials.gov, number NCT02885610.
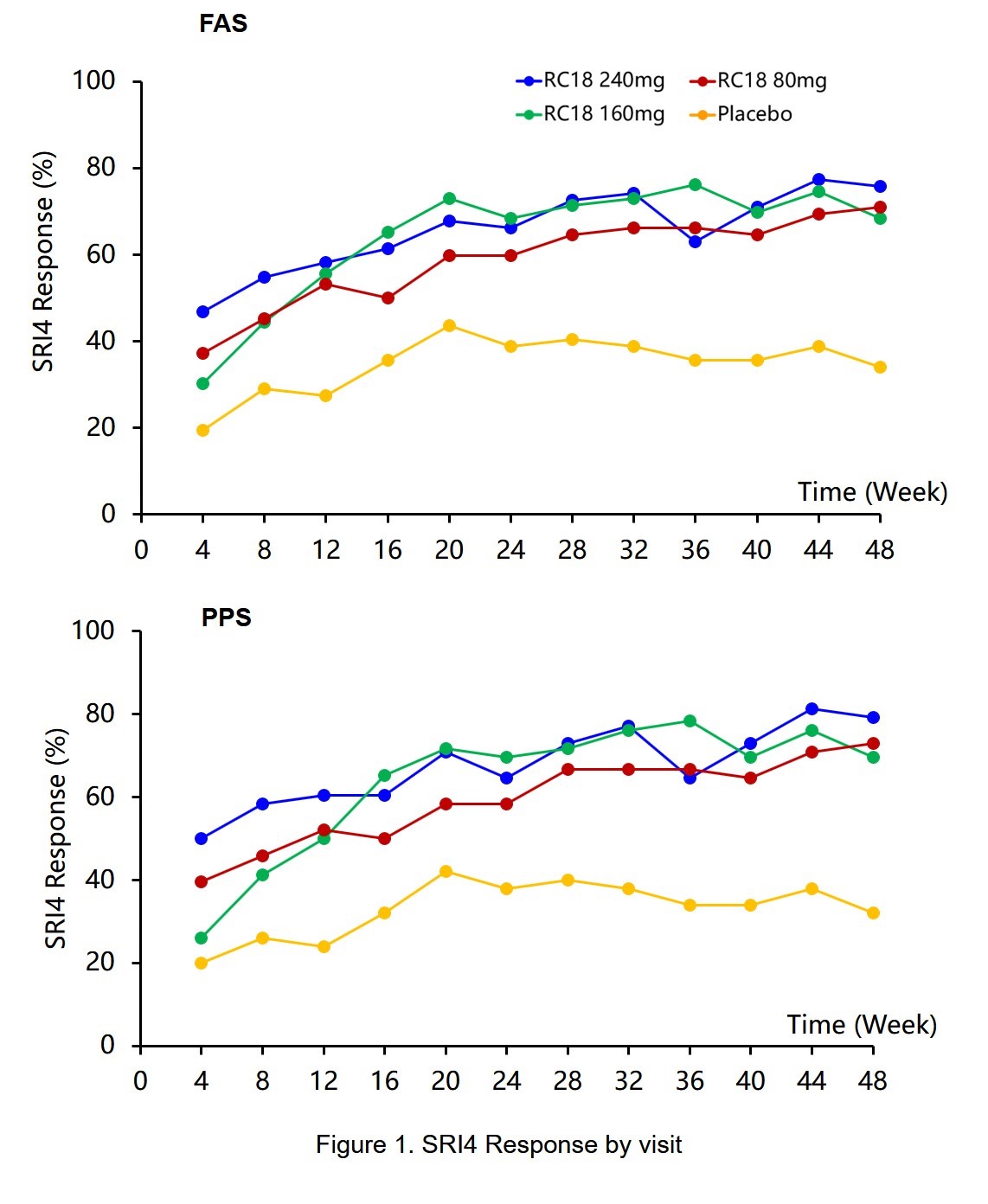
Results: 249 patients were randomized to receiving Telitacicept 80 mg (n=62), 160 mg (n=63), 240 mg (n=62) or placebo (n=62). Results from full analysis set (FAS) showed significantly higher response rates of SRI4 with Telitacicept 80mg (71.0%, p< 0.0001), 160 mg (68.3%, p=0.0001) and 240 mg (75.8%, p< 0.0001) than with placebo (33.9%) at Week 48; more patients had a reduction of ≥ 4 points in SELENA-SLEDAI score at Week 48 with Telitacicept 80mg (75.8%, p=0.003), 160 mg (77.8%, p=0.001) and 240 mg (79.0%, p< 0.001) than with placebo (50.0%); no worsening in PGA score was noted in more patients with Telitacicept 80mg (96.8%, p< 0.001), 160 mg (92.1%, p=0.013) and 240 mg (96.8%, p< 0.001) than with placebo (75.8%) at Week 48. Results from Per protocol set (PPS) were consistent with that from FAS. The incidences of AEs was 93.5%、92.1%、90.3%、82.3% in the Telitacicept 240mg, 160mg, 80mg and placebo group. There were 13 SAEs in 8 subjects treated with 240mg Telitacicept, 16 SAEs in 10 subjects treated with 160mg Telitacicept, 12 SAEs in 8 subjects treated with 80mg Telitacicept, 12 SAEs in 10 subjects treated with placebo, the incidences of SAEs were 12.9%, 15.9%,12.9%, 16.1% in the Telitacicept 240mg, 160mg, 80mg and placebo groups, respectively. The incidence of AEs and SAEs was similar across groups (p >0.05). There was 1 death in Telitacicept 240mg group which was considered not related to the study drug. The most common AEs were upper respiratory tract infection and injection site reactions. 11 pregnancies occurred during the study in subjects received Telitacicept (4 on 240mg, 3 on 160 mg and 4 on 80 mg) while no pregnancy occurred in the placebo group. 1 pregnancy resulted in live birth and 10 in elective termination.
Conclusion: This phase 2b trial in patients with active SLE treated with Telitacicept in combination with standard therapy met the SRI4 primary endpoint. Telitacicept was well tolerated in SLE patients.

To cite this abstract in AMA style:
Wu D, Li J, Xu D, Wang W, Li L, Fang J, Zhang F. A Human Recombinant Fusion Protein Targeting B Lymphocyte Stimulator (BlyS) and a Proliferation-Inducing Ligand (APRIL), Telitacicept (RC18), in Systemic Lupus Erythematosus (SLE): Results of a Phase 2b Study [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/a-human-recombinant-fusion-protein-targeting-b-lymphocyte-stimulator-blys-and-a-proliferation-inducing-ligand-april-telitacicept-rc18-in-systemic-lupus-erythematosus-sle-results-of-a-phase/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-human-recombinant-fusion-protein-targeting-b-lymphocyte-stimulator-blys-and-a-proliferation-inducing-ligand-april-telitacicept-rc18-in-systemic-lupus-erythematosus-sle-results-of-a-phase/