Background/Purpose
Socio-economic (SE) inequalities in health persist both between and within countries and even increased in the recent years. Therefore, it is important to explore whether country level factors may contribute to health inequities in patients with RA. The objectives of this study was to (1) investigate whether country level factors contribute to explain Disease Activity Score (DAS28) (2) explore whether uptake of biologic disease modifying anti-rheumatic drugs (bDMARDs) mediates the relationship between country welfare and DAS28.
Methods
Data from a cross-sectional multinational (17 countries) study (COMORA) was used. The outcome was DAS28. Contribution of country to DAS28 was explored in multivariable linear regression models, adjusting for potential confounders, using forward selection and accounting for multiple testing. The country with lowest DAS28 (Netherlands (NL)) was used as reference. Next, the country of residence was replaced by GDP (dichotomized in low and high GDP), to investigate the contribution of socio-economic welfare. Improvement in R2(model fit) of the two models that included either country or GPD was compared. Finally, the mediating role of uptake of bDMARDs in the relationship between GDP and DAS28 was explored by testing indirect effects.
Results
A total of 3920 RA patients from 17 countries (range 30-411) were included in COMORA dataset. Mean age was 56 y.o. (SD13), 82% females. Mean DAS28 was 3.7 (range 2.6 (NL) – 5.2 (Morocco)), and 32% of patients were currently treated with bDMARDs (range 3%(Uruguay) – 74% (UK)). Country differences in DAS28 varied from 0.2 (France) to 2.3 (Morocco) compared to NL, after adjustment for individual factors (Figure 1A). In societies with low GDP disease activity was on average 0.98 units higher, compared to high GDP countries (Figure 1B). Additional contribution of country to R2was 0.15 and of GDP 0.08. Seven percent of the differences in DAS28 between low and high GDP countries were mediated by (lower) uptake of bDMARDs (Figure 2).
Conclusion
Substantial differences in DAS28 between countries were observed after adjusting for individual factors. In countries with low GDP disease activity was higher than in countries with high GDP. Lower uptake of biologics mediated part of the relationship between (low) GDP and (high) disease activity. Inequities across countries should come at focus of international societies of rheumatology and policy-makers.
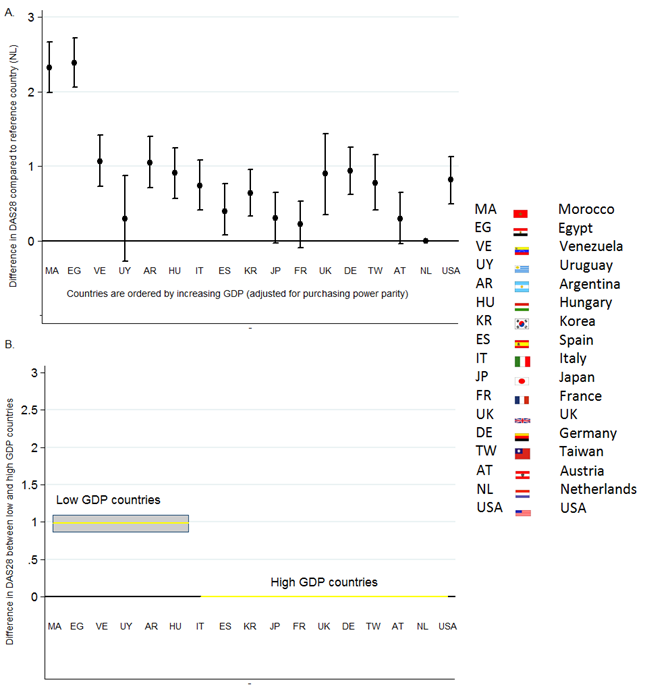
Figure 1. Differences in average DAS28 between individual countries (Figure 1A) and countries grouped by GDP (Figure 1B). Estimates are derived from models adjusted for age, gender, education, high rheumatoid factor or anti-citrullinated protein antibody, and comorbidities.
Disclosure:
P. Putrik,
None;
S. Ramiro,
None;
A. Keszei,
None;
I. Hmamouchi,
None;
M. Dougados,
None;
T. Uhlig,
None;
T. K. Kvien,
None;
A. Boonen,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/country-of-residence-and-its-wealth-determine-disease-activity-levels-in-ra-results-from-multi-national-study-across-17-countries-comora/