Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose Studies of ‘prevalent’ cohorts wherein most patients have longstanding disease at recruitment may underestimate mortality in systemic sclerosis (SSc) due to survivor bias. The aim of this study was to quantify mortality in Australian, Canadian and Spanish patients with SSc and to compare patients with prevalent and incident disease.
Methods We quantified mortality as Standardized Mortality Ratio (SMR) and Years of Life Lost (YLL) in each of the cohorts based on Australian Bureau of Statistics, Statistics Canada and Spain National Statistics Institute data for the general population, and percentage survival in the first decade of disease in the whole combined ‘prevalent’ cohort and a subset of patients recruited within 4 years of onset of disease (the combined ‘incident’ cohort). We determined a single primary cause of death (SSc or non-SSc related) and all other SSc organ involvement that contributed to death.
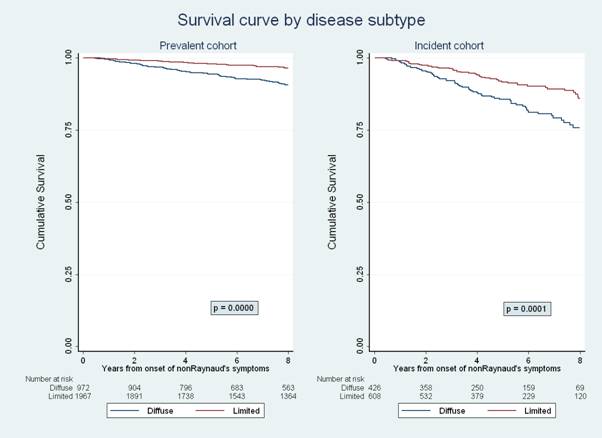
Results In the combined prevalent cohort of 3218 patients (1411 Australian, 1465 Canadian and 342 Spanish), 53% of the primary causes of 440 deaths (157 Australian, 213 Canadian and 70 Spanish) recorded were SSc related; the most common cause of SSc-related death was heart-lung disease (Table 1). Malignancy, atherosclerotic vascular disease and sepsis were the most common non-SSc related causes. SSc organ involvement contributed to 31% of these non-SSc related deaths. In multivariable regression, the predictors of mortality were male sex, older age at disease onset, diffuse subtype and presence of PAH, ILD, myocardial involvement, or renal crisis. The SMR and YLL were higher (Table 2) in Australian and Canadian incident cohorts compared with the respective prevalent cohorts. Survival was lower (Figure 1) in the combined incident cohort than the prevalent cohort.
Conclusion Mortality in Canadian, Spanish and Australian SSc patients is substantial. Our results suggest that prevalent cohorts underestimate mortality in SSc by failing to capture early deaths, particularly in diffuse disease. These findings provide a compelling rationale for establishing a large multi-national inception cohort of patients with SSc to more accurately quantify early mortality in this disease.
Table 1 Causes of SSc-related death
|
Organ system |
Australian Cohort 01/2007-03/2014 |
Canadian Cohort 01/2005-03/2014 |
Spanish Cohort 01/2000-03/2014 |
Combined cohort
|
||||
|
|
Principal Cause N=87 n(%) |
Contribu-ting cause N=157 n (%) |
Principal Cause N=94 n (%) |
Contribu-ting cause N=213 n (%) |
Principal cause N=52 n (%) |
Contribu-ting cause N=70 n (%) |
Principal cause N=233 n (%) |
Contribu -ting cause N=440 n (%) |
|
Heart and Lung |
74(85.0) |
44(28.0) |
57(60.6) |
55(25.8) |
35(67.3) |
12(17.1) |
166(71.2) |
111(25.2) |
|
PAH |
41(47.1) |
24(15.3) |
30(31.9) |
22(10.3) |
14(26.9) |
3(4.3) |
85(36.5) |
49(11.1) |
|
ILD |
19(21.8) |
20(12.7) |
17(18.1) |
33(15.5) |
14(26.9) |
9(12.9) |
50(21.5) |
62(14.1) |
|
PAH and ILD |
14(16.1) |
|
10(10.6) |
|
7(13.5) |
|
31(13.3) |
|
|
Myocardial involvement |
2(2.3) |
0(0) |
8(8.5) |
7(3.3) |
10(19.2) |
8(11.4) |
20(8.6) |
15(3.4) |
|
Pericardial involvement |
0(0) |
3(1.9) |
4(4.3) |
5(2.3) |
0(0) |
3(4.3) |
4(1.7) |
11(2.5) |
|
Renal crisis |
4(4.6) |
1(0.6) |
9(9.6) |
6(2.7) |
2(3.8) |
3(4.3) |
15(6.4) |
10(2.3) |
|
Gut involvement |
6(6.9) |
14(8.9) |
14(14.9) |
17(8.0) |
4(7.7) |
13(18.6) |
24(10.3) |
44(10.0) |
|
Sepsis due to ischemic digit or decubitus ulcer |
2(2.3) |
22(14.0) |
1(1.1) |
6(2.8) |
1(1.9) |
13(18.6) |
4(1.7) |
41(9.3) |
Table 2 A comparison of mortality in ‘prevalent’ and ‘incident’ cohorts
|
|
Australian Patients 01/2007-12/2012 |
Canadian Patients 01/2005-12/2012 |
Spanish Patients 01/2000-12/2012 |
|||
|
|
‘Prevalent’ cohort n=1252 |
‘Incident’ cohort n=339 |
‘Prevalent’ cohort n=1132 |
‘Incident’ cohort n=405 |
‘Prevalent’ cohort n=342 |
‘Incident’ cohort n=183 |
|
Number of deaths |
110 |
27 |
151 |
53 |
58 |
32 |
|
SMR(95%CI) Women Men Overall |
2.6(2.1-3.1) 4.2(2.4-5.9) 2.8(2.4-3.3) |
2.4(1.2-3.5) 9.1(3.7-14.5) 3.4(2.3-4.5) |
3.3 (2.7-3.9) 5.9 (3.9-7.9) 3.7 (3.2-4.2) |
4.2 (2.9-5.5) 6.8 (3.1-10.4) 4.7 (3.6-5.7) |
4.1(3.0–5.3) 9.5(3.6–15.4) 4.6(3.7–5.5) |
3.3(2.0–4.5) 8.4(1.7–15.1) 3.8(2.8–4.9) |
|
YLL (years) Women Men |
11.9 17.2 |
11.3 25.8 |
19.8 16.7 |
21.1 19.7 |
22.4 24.4 |
16.4 25.7 |
Figure 1 Survival curves in combined cohorts
Disclosure:
Y. Hao,
None;
M. Hudson,
None;
P. Carreira,
None;
W. Stevens,
None;
C. Rabusa,
None;
S. Tatibouet,
None;
L. Carmona,
None;
B. E. Joven,
None;
S. Proudman,
None;
M. Baron,
None;
M. Nikpour,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/early-mortality-in-australian-canadian-and-spanish-scleroderma-patients-rationale-for-establishing-a-multi-national-inception-cohort-of-patients-with-systemic-sclerosis/