Background/Purpose: There is need to improve the magnitude and duration of treatment effects of exercise therapy (ET) for patients with knee osteoarthritis (KOA). There is conflicting evidence that manual therapy (MT) can enhance treatment effect magnitude of ET for pain and function. The use of booster treatment sessions have also been suggested to improve sustainability of these treatment effects, but evidence is lacking. The aims of the study were to: 1) determine if adding MT to ET programs would result in an additive treatment effect on pain and function, and 2) determine if use of booster treatment sessions would result in greater sustainability of these effects in patients with KOA.
Methods: Multi-center randomized clinical trial, including three clinical sites from different regions of the United States. 300 subjects (mean age = 58 ± 9 years; 199 female) meeting the ACR clinical criteria for KOA were randomly allocated to 1 of 4 groups; 1) ET- no booster, 2) ET + booster, 3) MT+EX-no booster, and 4) MT+Ex + booster. Subjects not receiving booster sessions received 12 treatment sessions in 9 weeks. Subjects receiving booster sessions received 8 treatment sessions in 9 weeks then received 4 additional booster treatment sessions distributed over the remaining year. Primary outcome measure was the WOMAC total score. Secondary outcome measures included the numeric knee pain rating, the Timed Up and Go (TUG) test, the 30 sec. chair rising test, and the 40m walk test. Outcome measures were obtained at baseline, 9 weeks, and 1 year. Data was analyzed using a repeated measures linear mixed model of treatment effect and the treatment group by time interaction was performed, adjusting for treatment site location and bilateral knee involvement. Statistical significance was α = .05.
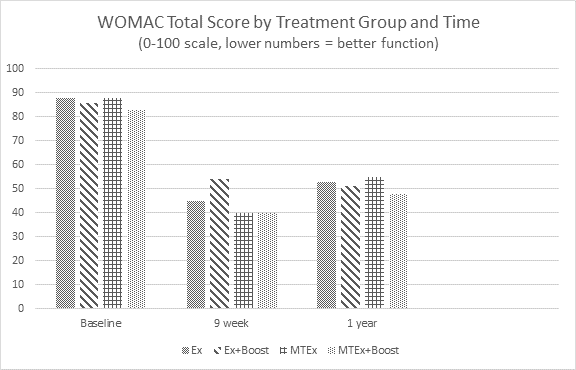
Results: The figure summarizes the WOMAC total scores at each time point. There were no statistical or clinically meaningful differences between treatment groups at either follow-up time point. There was no significant treatment group by time interaction. All treatment groups demonstrated meaningful changes in clinical outcome from baseline to the 9 week follow-up (within group effect sizes range = .69 to 1.2; percent change from baseline range = 37%-54%) which was also maintained over the 1 year follow-up period (within group effect sizes range = .70 to .85; percent change from baseline range = 37%-40%). Similar results were observed for all other outcome measures.
Conclusion: Adding MT to ET did not increase the magnitude of treatment effect and use of booster sessions did not exhibit superior sustainability of treatment effects over time. All four treatment approaches tested in this study yield moderate to large improvements in pain and function that were sustained over a one year period.
Disclosure:
G. K. Fitzgerald,
None;
J. Fritz,
None;
J. Childs,
None;
G. P. Brennan,
None;
D. P. Landsittel,
None;
B. Neilson,
None;
A. Gil,
None;
J. H. Abbott,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/exercise-manual-therapy-and-use-of-booster-sessions-in-physical-therapy-for-knee-oa-a-multi-center-randomized-clinical-trial/