Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: No single gold standard for remission is available for rheumatoid arthritis (RA). All available descriptions, including 2 proposed by an ACR/EULAR committee, allow residual joint abnormalities and RA symptoms. Relatively little information is reported concerning these abnormalities in patients who meet various descriptions of remission.
Methods: The ESPOIR cohort of 734 patients with complete 6-month data was analyzed to identify those in remission according to 8 descriptions, 4 requiring a formal joint count: disease activity score (DAS28) ≤2.6, clinical disease activity index (CDAI) ≤2.8, and the 2 proposed by ACR/EULAR – Boolean dichotomy with tender joint count (TJC28), swollen joint count (SJC28), C-reactive protein (CRP) and patient global estimate (PATGL) all ≤1, and simplified disease activity index (SDAI) ≤3.3. Four additional descriptions are based on routine assessment of patient index data (RAPID3), an index of patient-reported function, pain and PATGL with remission (RAPID3R) described by a score ≤3 (0-30 scale), and 3 more stringent definitions that add a careful joint examination and physician global estimate (DOCGL): RAPID3R+J1 (RAPID3 ≤3 and £1 swollen joint); RAPID3R+J1D1 (RAPID3 ≤3, £1 swollen joint and DOCGL ≤1); and RAPID3R+J0D1 (RAPID3 ≤3, no swollen joint and DOCGL ≤1). Proportions of patients with TJC28, SJC28, CRP, DOCGL, PATGL, pain or fatigue >1, or HAQ function (FN) >0.5, and specific swollen joints (n=28) were computed for each remission description.
Results: Boolean dichotomy and RAPID3R+J0D1 indicated 13% of all patients in remission vs 16–19% by SDAI, CDAI, RAPID3R+J1 and RAPID3R+J1D1. RAPID3R (26%) and DAS28 (32%) were least stringent. TJC28 >1 was seen in 0% by Boolean criteria (by definition) vs 3–11% by SDAI, CDAI, DAS28; 13–16% by RAPID3R+J1, RAPID3R+J1D1, RAPID3R+J0D1; and 24% by RAPID3R. SJC28 >1 was seen in 0% by Boolean criteria, RAPID3R+J1, RAPID3R+J1D1 and RAPID3R+J0D1 (by definition); 2% by CDAI and SDAI; 16% by DAS28; and 27% by RAPID3R. CRP >1 was seen in <8%, and HAQ-FN >0.5 in 2–12% by all 8 descriptions. PATGL >1 was seen in 10–21% by all but Boolean (0% by definition) and DAS28 (49%); pain >1 in 9–23% by all but DAS28 (46%); and fatigue >1 in 47–65% by all 8 descriptions. Knees, shoulders and elbows were involved in <5% of patients by all 8 descriptions; wrists in <6%, MCPs in <9% and PIPs in <5%, except by DAS28 and RAPID3R. Most residual joint involvement was of MCPs or PIPs.
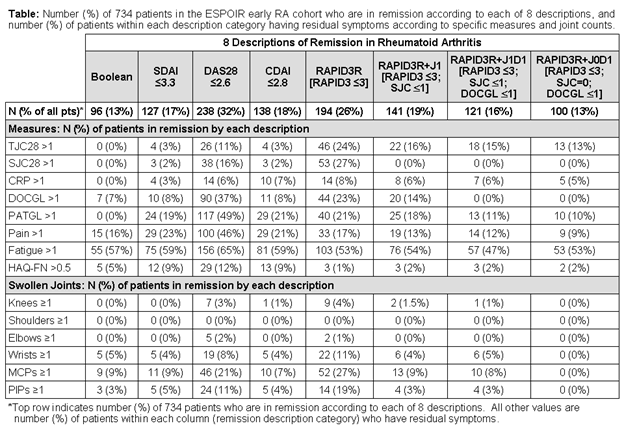
Conclusion: At least 9% of patients in remission by any description had pain, and at least 47% fatigue. RAPID3R and DAS28 had the largest proportions of patients with residual abnormalities, while CDAI and stringent RAPID3-based remission descriptions are similar to the 2 proposed by ACR/EULAR. RAPID3-based descriptions do not require formal joint counts or laboratory data, but do require DOCGL and careful joint examination, and could be feasible in usual care.
Disclosure:
I. Castrejón,
None;
M. Dougados,
None;
B. Combe,
None;
F. Guillemin,
None;
B. Fautrel,
None;
T. Pincus,
None.
« Back to 2012 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/residual-disease-activity-in-patients-with-early-rheumatoid-arthritis-who-were-classified-as-being-in-remission-according-to-8-different-descriptions-post-hoc-analysis-of-the-etude-et-suivi-des-polya/