Session Information
Session Type: Abstract Submissions (ACR)
Treatment Delays and Worse Outcomes Associated with Low Socioeconomic Status in Rheumatoid Arthritis
Background/Purpose: Prompt and routine care in rheumatoid arthritis (RA) is critical for best outcomes. Low socioeconomic status (SES) RA patients use fewer health services and have higher disease activity. We sought to examine the role of SES, distance to the rheumatologist (DTR), and delays in DMARD treatment as determinants of outcome in RA.
Methods: RA outpatients were recruited from public, private, military and Veteran’s Affairs rheumatology clinics. The recruitment period spanned nearly 15 years. We assessed SES based on education, occupation and income using the Nam & Powers scale. The time from RA symptom onset to DMARD initiation (DMARD lag) was determined by self-report of the two dates. The distance from a patient’s address to the rheumatologist was obtained using Google Maps. We examined three specific clinical outcomes in RA: disease activity, determined by DAS28ESR; joint damage, determined from hand radiographs using the Sharp score; and physical disability, determined by the Modified Health Assessment Questionnaire (MHAQ). We used linear regression models to examine the association of the clinical outcomes with SES, DTR, and DMARD lag, adjusting for other confounders such as age, sex, ethnicity and duration of RA.
Results: We recruited 1,209 RA patients, 1159 of whom had received DMARD treatment. Average DMARD lag was 6.9 ± 8.9 years. Greater DMARD lag was associated with older age (P≤0.001), longer disease duration (P≤0.001) and worse status on all three clinical outcomes (P≤0.001). Lower SES was associated with a longer DMARD lag (beta coeff. -0.120, P≤0.001) and a shorter DTR (beta coeff. 0.261, P≤0.001). On average, patients with lower SES waited 8.5 ± 10.2 years after onset of RA symptoms to begin DMARD treatment, which was significantly longer than those in middle and upper SES tertiles who waited 6.1 ± 7.9 years (P=0.002) and 6.1 ± 8.6 years (P=0.009), respectively. Adjusting for confounders including DTR and DMARD lag, SES remained inversely associated with DAS28ESR (beta coeff. -0.282, P≤0.001), Sharp score (beta coeff. -0.135, P≤0.001) and MHAQ (beta coeff. -0.296, P≤0.001).
Conclusion: Low SES RA patients experience a significantly greater delay in DMARD treatment. Low SES and greater DMARD lag were independently associated with worse clinical outcomes, despite adjusting for potential barriers to care such as distance to the rheumatologist and other confounders. Strategies to reduce treatment delay in low SES RA patients are needed.
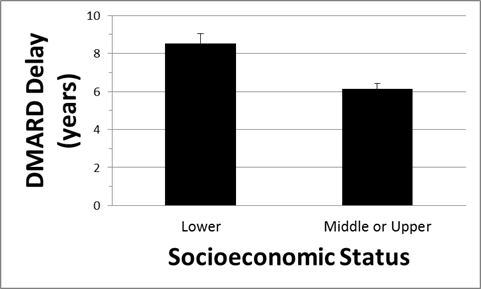
Figure 1. Average time from RA symptom onset to DMARD initiation according to socioeconomic status.
Disclosure:
E. Molina,
None;
J. F. Restrepo,
None;
I. del Rincon,
None;
D. Battafarano,
None;
A. Escalante,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/treatment-delays-and-worse-outcomes-associated-with-lower-socioeconomic-status-in-rheumatoid-arthritis/