Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Although both exercise therapy and manual therapy have evidence supporting their effectiveness in people with hip and knee osteoarthritis (OA), few clinical trials have reported their incremental effectiveness compared with usual medical care, or their long-term effects.
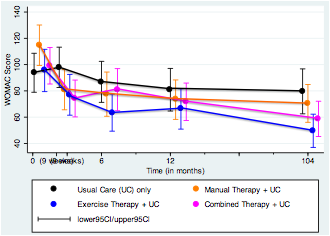
Methods: In this randomized controlled trial with 2-year follow-up, adults meeting the American College of Rheumatology criteria for hip or knee OA were randomly allocated to receive either a] exercise therapy; b] manual therapy; c] combined exercise therapy and manual therapy; or d] no trial intervention in addition to usual medical care. Groups a-c were provided 10 treatment sessions: 7 sessions within the first 9 weeks plus 3 booster sessions (2 at 4 months and 1 at 13 months). Assessors blinded to group allocation reassessed participants at 2 years. The primary outcome measures were the Western Ontario and McMaster (WOMAC) osteoarthritis index (24 questions, 0-10 scale, total range 0-240) and physical performance tests (timed up-and-go, 40m fast-paced walk, 30 second sit-to-stand).
Results: 186 (90.3%) of 206 participants recruited were retained at 2 years follow-up. At baseline, mean age was 66 years (range 37 to 92) and mean WOMAC was 100.8 (SD 53.8). Missing data were replaced using multiple imputation. Intention-to-treat analysis of covariance (ANCOVA) showed improvements in WOMAC at 2 years were superior for all three intervention groups compared with the usual care group (2-sided p<0.05). Participants receiving exercise therapy in addition to usual care showed gains of 31.7 WOMAC points (95% CI 10.0, 53.3); effect size 0.57 (Cohen’s d; 95% CI .17, .97). Participants receiving manual therapy in addition to usual care showed gains of 30.1 (8.9, 51.3); effect size 0.55 (.16, .94). Participants receiving combined exercise therapy and manual therapy in addition to usual care did not meet the a priori threshold for clinical significance (28 points), but were 26.2 (6.1, 46.3) WOMAC points better than usual care only, for a clinically significant effect size of 0.52 (.11, .91). The exercise therapy group showed greater mean changes on most physical performance tests than did the other groups.
Conclusion: Both exercise physiotherapy and manual physiotherapy provided incremental benefit over usual care alone at 2 years follow-up. Physical performance test outcomes significantly favoured the exercise therapy group.
Disclosure:
J. H. Abbott,
None;
C. Chapple,
None;
D. Pinto,
None;
A. Wright,
None;
J. C. Theis,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/exercise-therapy-andor-manual-therapy-for-hip-or-knee-osteoarthritis-2-year-follow-up-of-a-randomized-controlled-trial/