Session Information
Date: Saturday, March 21, 2026
Title: Plenary Abstract Session III
Session Time: 11:00AM-11:15AM
Background/Purpose: Patients with systemic autoimmune diseases like childhood-onset systemic lupus erythematosus (cSLE) and juvenile dermatomyositis (JDM) typically receive oral glucocorticoids at the onset of their diagnosis and during periods of flare. The duration of therapy ranges from weeks to months, placing them at risk for glucocorticoid-induced adrenal insufficiency (GIAI) and adrenal crisis. This risk is often under-recognized, leading to a delay in administration of stress-dose steroids (SDS), which can be fatal. This quality improvement study aims to explore if: 1) providing GIAI education to rheumatologists increases the frequency of documentation of patient risk status for GIAI and 2) if clinical decision support tools embedded into the electronic health record (EHR) increase administration of SDS when clinically indicated in the Emergency Department (ED) for these patients.
Methods: The study team developed several EHR-integrated clinical decision support tools (including SDS action plan), held educational sessions with the rheumatology division as well as other key stakeholder groups, and engaged in multiple Plan-Do-Study-Act (PDSA) cycles throughout the study period. The patient population included patients diagnosed with JDM or cSLE at our institution between July 2023 and September 2025. The primary outcome measure was percentage of ED encounters within the study population where SDS were appropriately administered, and the primary process measure was the percentage of eligible patients with GIAI risk status and SDS action plan documented within their charts during the study period.
Results: There were 68 total new diagnoses of cSLE (n=43, 63%) and JDM (n=25, 37%) identified during the 14-month study period. By study end, 62% (n=42) had a documented stress-dose steroid action plan (Figure 2). Additionally, rates of clinically indicated stress-dose steroid administration in the ED rose from a baseline of 0% (0/5) to 79% (15/19) over the course of the study, including administration of SDS in 100% (5/5) of the ED visits during the last 2 months of the study period (Table 1).
Conclusion: In this patient population at high risk for GIAI, provider education and development of EHR-embedded clinical decision support tools led to the documentation of risk status for the majority of eligible patients. Study patients also received remarkably high rates of stress-dose steroids in the ED when clinically indicated, with no episodes of unrecognized or delayed treatment of adrenal crisis during the study period. This represents a promising and effective strategy for mitigating iatrogenic harm in pediatric rheumatology patients, and expansion to other patient populations merits consideration.
Figure 1.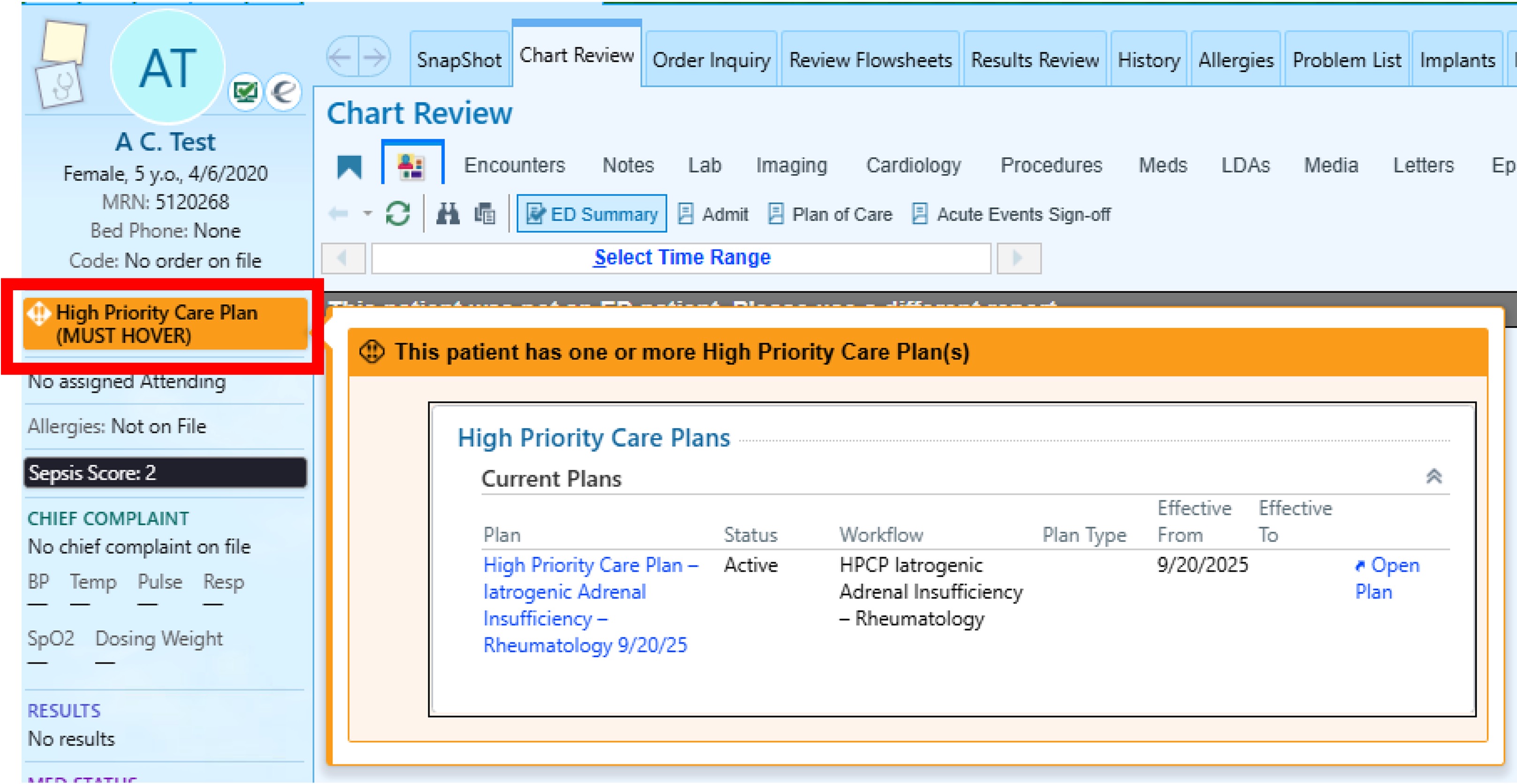 Banner within EHR, labeled “High Priority Care Plan”, alerting providers to review action plan (© 2025 Epic Systems Corporation)
Banner within EHR, labeled “High Priority Care Plan”, alerting providers to review action plan (© 2025 Epic Systems Corporation)
Figure 2.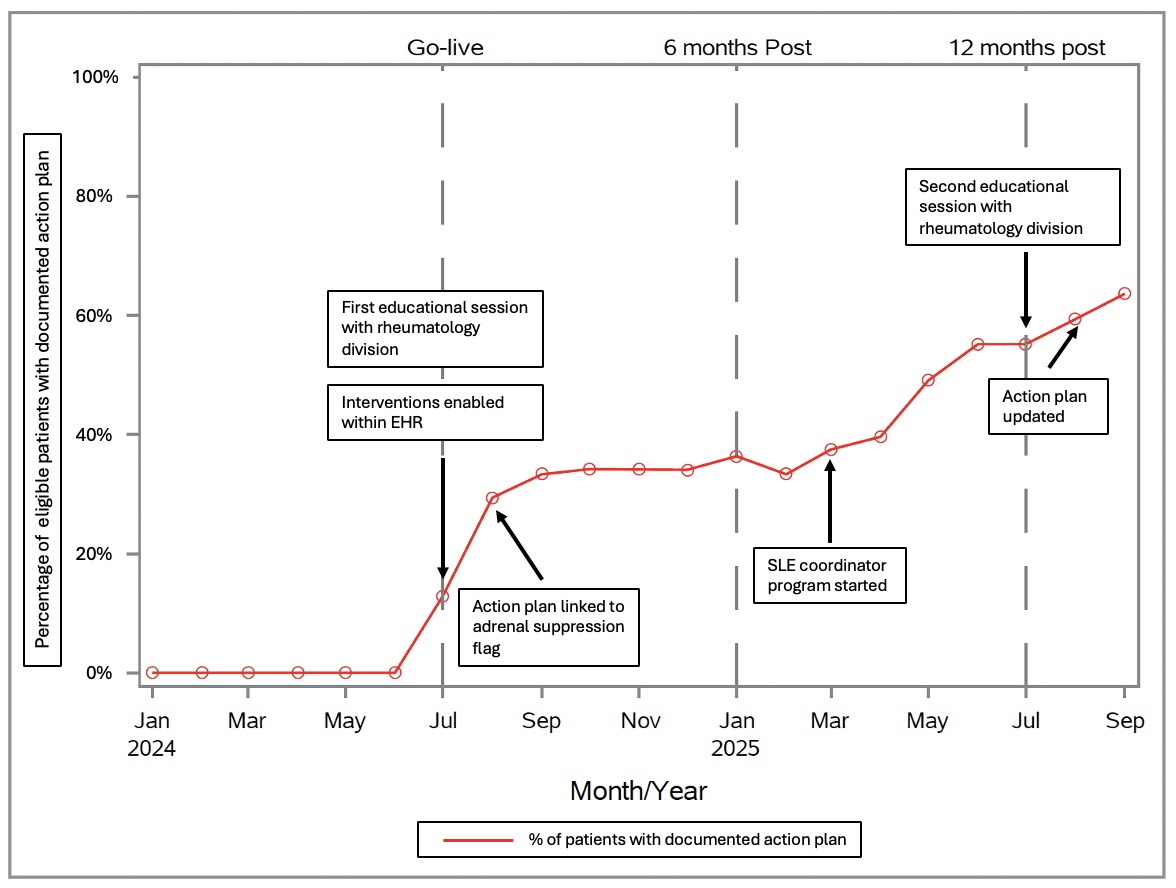 Run chart of proportion of patients with documented action plan within their chart over the 14 month study period, including 6 months of baseline prior to intervention start
Run chart of proportion of patients with documented action plan within their chart over the 14 month study period, including 6 months of baseline prior to intervention start
Table 1. 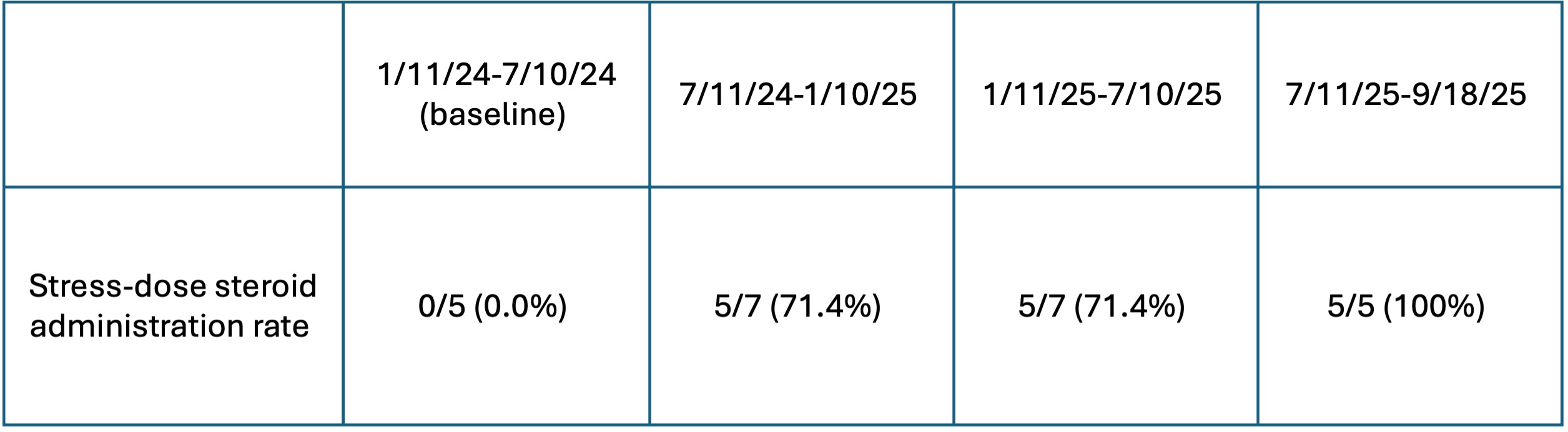 Rate of clinically indicated stress-dose administration during institutional ED visits for patients within study population, as tabulated in 6 month increments over the course of the study. Clinical indication for stress-dose steroids determined by manual chart review.
Rate of clinically indicated stress-dose administration during institutional ED visits for patients within study population, as tabulated in 6 month increments over the course of the study. Clinical indication for stress-dose steroids determined by manual chart review.
To cite this abstract in AMA style:
Schildt E, Lynch H, Rosenwasser N, Shenoi S, Rutman L, Gupta M. Improving Recognition and Management of Glucocorticoid-Induced Adrenal Insufficiency in Pediatric Rheumatology Patients [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/improving-recognition-and-management-of-glucocorticoid-induced-adrenal-insufficiency-in-pediatric-rheumatology-patients/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/improving-recognition-and-management-of-glucocorticoid-induced-adrenal-insufficiency-in-pediatric-rheumatology-patients/