Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose: SLE leads to vascular compromise in multiple organs, including brain, leading to parenchymal infiltration. We have demonstrated increased permeability of the blood-brain-barrier (BBB) in SLE. A murine SLE study found infiltrates in CSF with intact BBB, driving inquiry of blood-CSF barriers (BCSFB) including choroid plexus (CP). The CP has fenestrated capillaries and an epithelium regulating exchange with ventricular CSF. Compromise of the BCSFB may be pathogenic for multiple sclerosis (MS) since MRI reveals periventricular gradients of T1 abnormality. Studies of the BCSFB in humans with SLE are lacking. We investigate alteration of the BCSFB in SLE and MS including CP volume and blood flow, and periventricular gradients of abnormality of normal-appearing white matter (NAWM). We include MS patients as positive controls to explore differences between autoimmune conditions.
Methods: Preliminary analysis included 18 SLE (15F, 17.4 (4.2) yrs), 10 MS (9F, 19.2 (3.5) yrs), and 35 healthy controls (HC, 25F, 19.5 (4.3) yrs). MRI included quantitative susceptibility mapping (QSM) and SyMRI (relaxometry, myelin concentration (MyC), tissue segmentation). ITK-SNAP provided ventricle segmentation iteratively dilated to make 50, 1-mm-thick, zones in NAWM (Fig. 1D). We extracted mean values of T1, T2, proton density (PD), MyC, and susceptibility per zone. A linear fit of HC values: intercept + sex + age + age^2, provided reference to describe deviations of SLE and MS values from HC as z-scores. We compared mean z-scores for MS and SLE vs. periventricular distance. We assessed CP volume and perfusion dynamics via arterial spin labeling (ASL). ASCHOPLEX segmented the CP. Dynamic perfusion signal, fitted to a model, provided arrival time and blood flow at the CP. We compared group volume, arrival time, and blood flow.
Results: T1 was elevated vs. HC for MS and SLE. MS had a gradient in T1, lacking in SLE. T2 had a similar pattern of abnormality. PD was elevated at the surface for both SLE and MS, but MS was more elevated with a steeper gradient (Fig. 1). MyC was diminished for both groups with greater abnormality for MS at the surface with steeper gradient. Susceptibility had a pattern like myelin for MS, but SLE showed an increase at middle distances (Fig. 2). CP volume, as % parenchymal volume, was significantly greater for SLE vs. HC or MS groups (Fig.3). Arrival time and blood flow did not differ significantly between groups.
Conclusion: Our results indicate abnormality of all relaxometry and susceptibility metrics close to the ventricular surface for MS patients with gradients toward HC values (z~0) with increasing distance. This expands published findings for T1 in MS. SLE also exhibits abnormality throughout NAWM, but some metrics (myelin, T1, T2, PD) have near normal values close to the ventricles with gradients of opposite direction to MS. Such findings might suggest that SLE and MS have different mechanisms for infiltration. We observed significantly increased CP volume for SLE but not for MS, suggesting differences in pathophysiology. Evidence for a CP route of brain infiltration could realign phenotyping of SLE and MS and drive targeted therapies.
Figure 1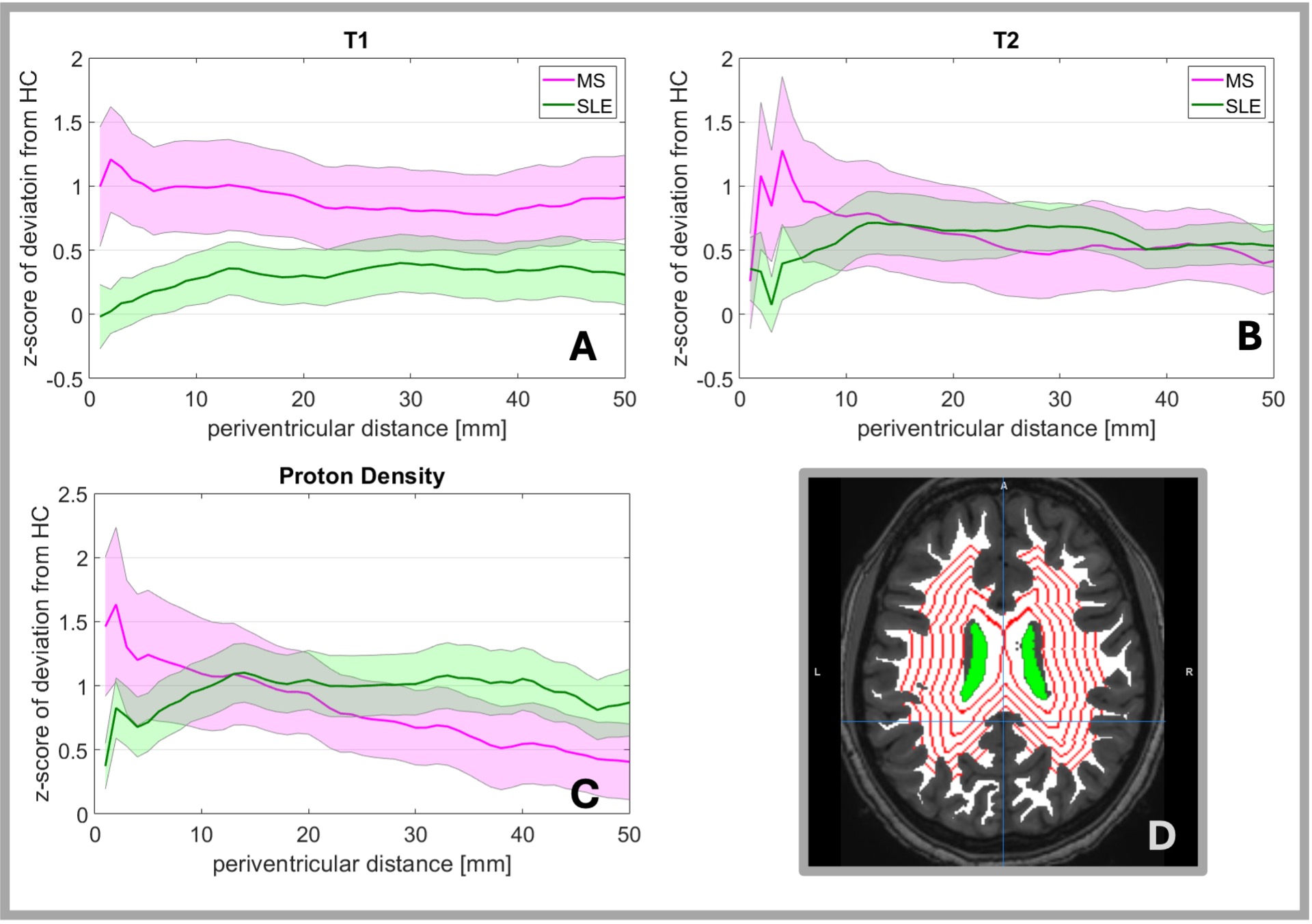 Periventricular gradients of abnormality (mean z-score of deviation from healthy control references) of A) T1, B) T2, and C) Proton Density. Shaded areas depict standard error. D) illustrates 1 mm thick zones at 5 mm intervals from the ventricular surface (green area).
Periventricular gradients of abnormality (mean z-score of deviation from healthy control references) of A) T1, B) T2, and C) Proton Density. Shaded areas depict standard error. D) illustrates 1 mm thick zones at 5 mm intervals from the ventricular surface (green area).
Figure 2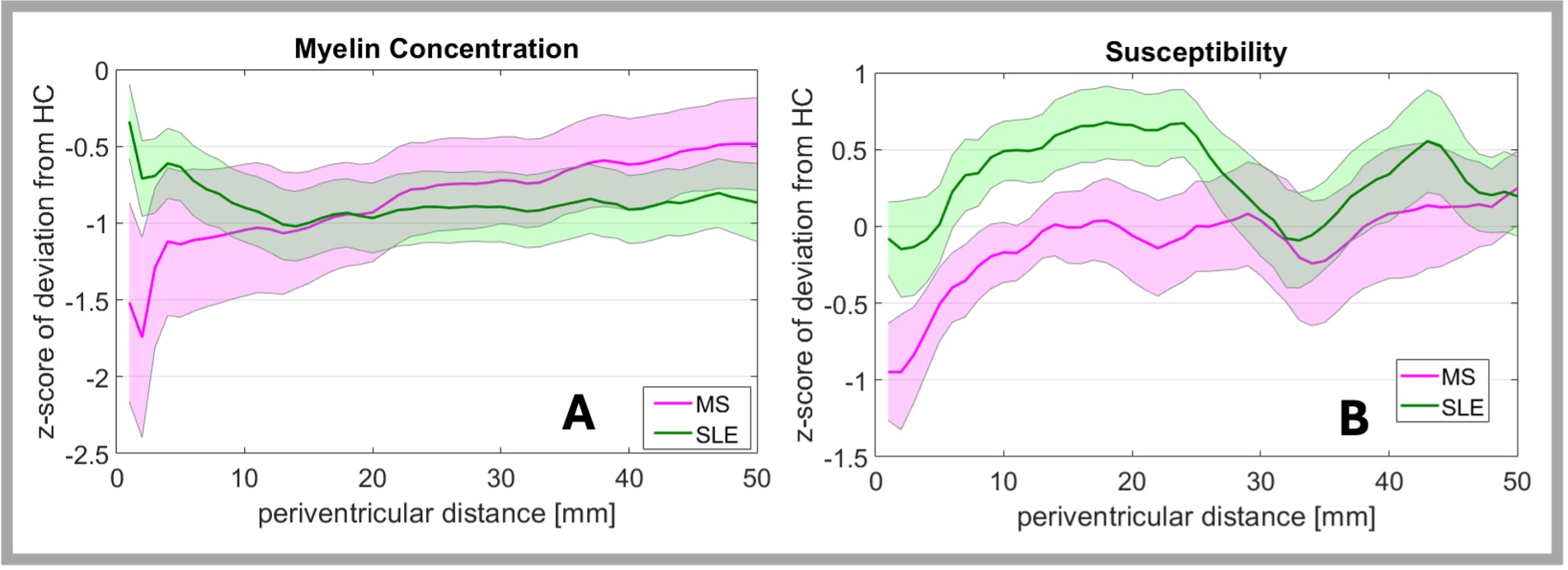 Periventricular gradients of abnormality (z-score of deviation from healthy control references) of A) Myelin Concentration, B) Susceptibility, and C) quantitative anisotropy. D) shows ChP flow dynamics. Shaded areas depict standard error.
Periventricular gradients of abnormality (z-score of deviation from healthy control references) of A) Myelin Concentration, B) Susceptibility, and C) quantitative anisotropy. D) shows ChP flow dynamics. Shaded areas depict standard error.
Figure 3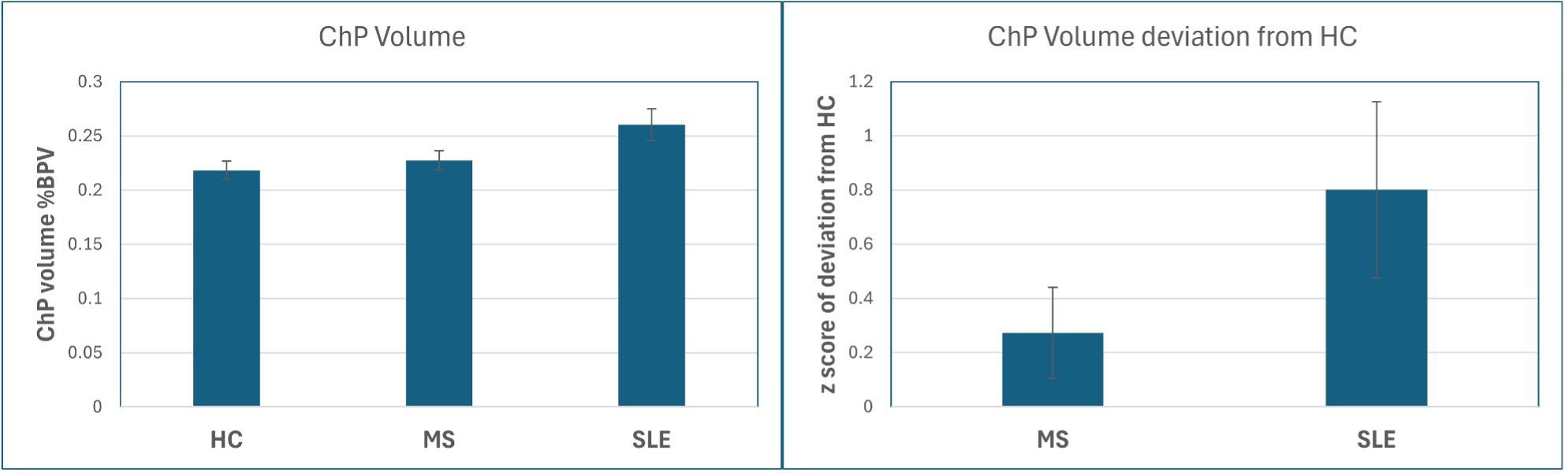 Choroid Plexus volume as percent of brain parenchymal volume. comparisons. Left: mean by group. Right: z-score of deviation from HC. Error bars depict standard error.
Choroid Plexus volume as percent of brain parenchymal volume. comparisons. Left: mean by group. Right: z-score of deviation from HC. Error bars depict standard error.
To cite this abstract in AMA style:
DiFrancesco M, Wilson E, Brunner H. The Blood-CSF-Barrier in SLE: Volume and Blood Flow of the Choroid Plexus and Periventricular Tissue Abnormality Gradients [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/the-blood-csf-barrier-in-sle-volume-and-blood-flow-of-the-choroid-plexus-and-periventricular-tissue-abnormality-gradients/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-blood-csf-barrier-in-sle-volume-and-blood-flow-of-the-choroid-plexus-and-periventricular-tissue-abnormality-gradients/