Session Information
Session Time: 5:00PM-6:00PM
Background/Purpose: Cumulative social disadvantage has been associated with persistent disease activity among children with juvenile idiopathic arthritis (JIA). Resilience is defined as the ability to adapt positively to adversity and has been associated with improved health-related quality of life in youth with JIA. Resilience can be measured at the individual (personal traits such as coping skills) or socioecological (external supports such as family, peers, or community resources) levels, but its potential role in mitigating health disparities related to cumulative social disadvantage has not been studied.
Methods: Individual (as measured by the Connor-Davidson Resilience Scale-10 [CD-RISC-10]; range 0-40) and socioecological (as measured by the Child and Youth Resilience Measure-17 [CYRM-R 17]; range: 17-85) resilience measures were collected in a cohort with existing JIA at the University of California, San Francisco (UCSF). The cumulative social disadvantage score (CSDS) was defined by one point for each of the following parameters (range: 0-3): 1) household income < $50,000/year, 2) public or no insurance, and 3) guardian education level of high school or less. Disease activity was measured at the corresponding clinical visit using the clinical Juvenile Arthritis Disease Activity Score (cJADAS)-10 (range: 0-30), comprised of physician global (0-10), patient/parent global (0-10), and joint count (0-10). We calculated summary statistics, including mean/median resilience and disease activity scores. We assessed correlation between CSDS, resilience, and disease activity using Pearson’s or Spearman’s correlation tests, as appropriate. To explore whether resilience modifies the relationship between CSDS and disease activity, we dichotomized resilience measures into high vs. low groups, and then used scatterplots to qualitatively compare the correlation between CSDS and disease activity.
Results: In total, 14 subjects with JIA completed resilience questionnaires (Table 1). 43% of the cohort experienced no social disadvantage (CSDS=0). Among those with CSDS > 1, public insurance was the most common parameter. Socioecological and individual resilience measures were highly correlated (r=0.7, p=0.005). CSDS and disease activity were weakly negatively correlated (r=-0.39, p=0.17), though this did not reach statistical significance (Figure 1). Among participants with CSDS scores of 0 or 1, high resilience was correlated with lower disease activity. In contrast, among those with CSDS scores of 2 or 3, higher resilience appeared to correspond with higher disease activity (Figure 2).
Conclusion: Although resilience was not statistically significantly associated with CSDS or disease activity, preliminary trends suggest that it may modify the relationship between social disadvantage and disease activity among youth with lower CSDS exposure. We plan to continue resilience questionnaire collection to assess the robustness of our findings and to conduct semi-structured qualitative interviews with youth with JIA and their guardians to contextualize these themes.
Demographic and clinical characteristics of the cohort 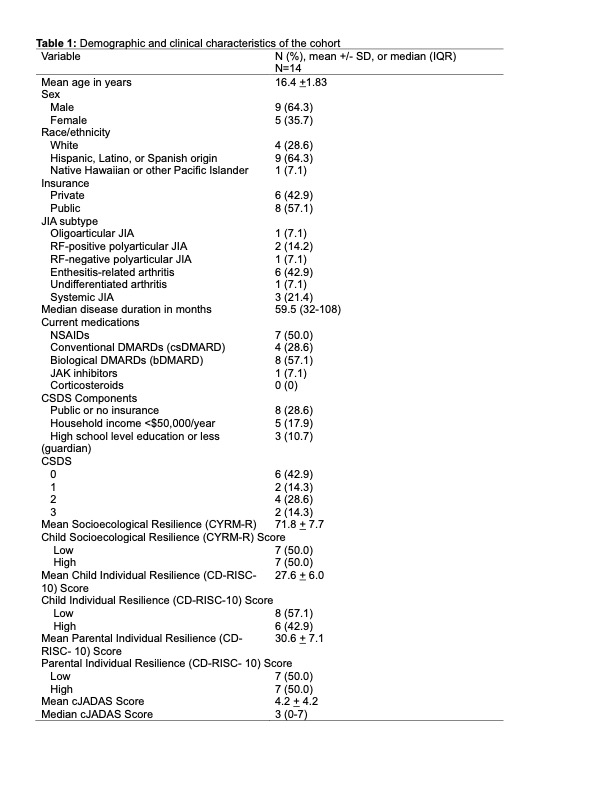
Correlation between cumulative social disadvantage (CSDS) and disease activity (as measured by the clinical Juvenile Arthritis Disease Activity Score [cJADAS]-10) in 14 youth with JIA (r = -0.39, p=0.17). 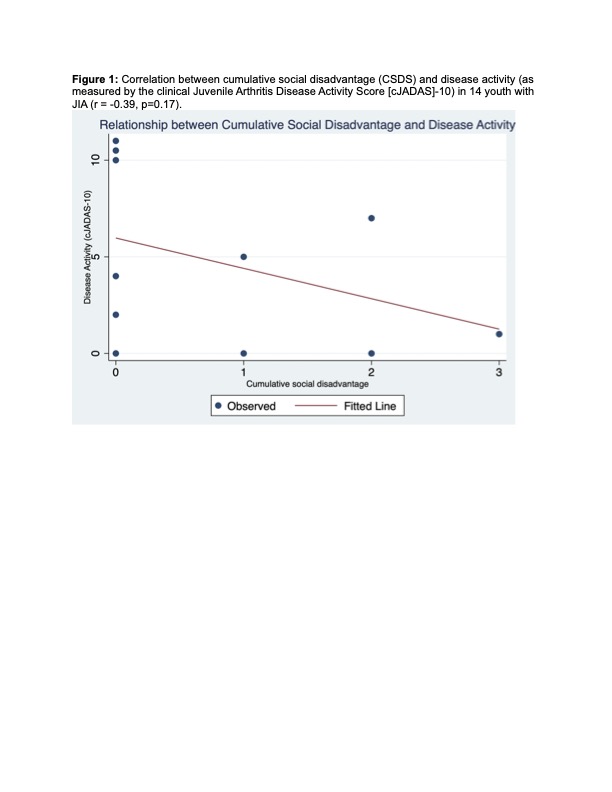
Correlation between cumulative social disadvantage (CSDS) and disease activity (as measured by the clinical Juvenile Arthritis Disease Activity Score [cJADAS]-10) stratified by resilience. Panel A: High versus low socioecological resilience (as measured by the CYRM-R-17). Panel B: High versus low individual resilience (as measured by the CD-RISC-10). 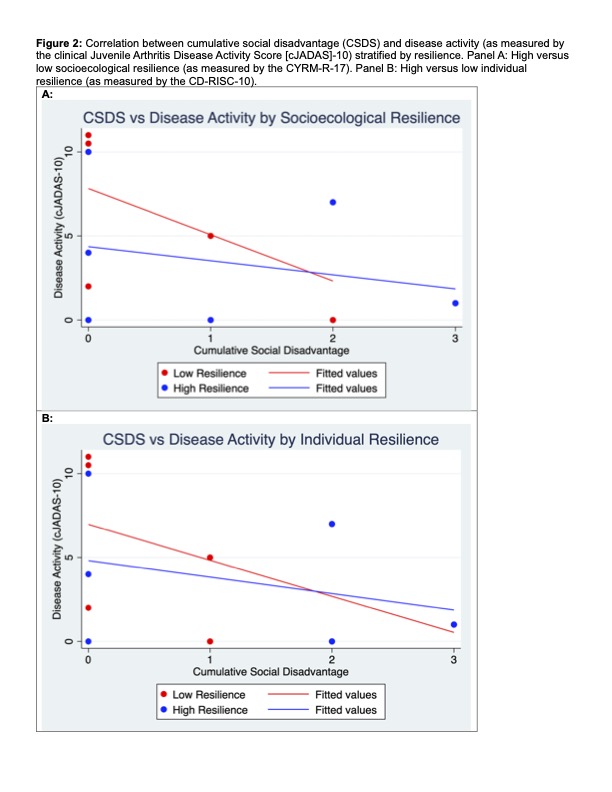
To cite this abstract in AMA style:
Soulsby W, Boscardin J, Knight A, Horton D, Toupin-April K, von Scheven E. Resilience, Cumulative Social Disadvantage, and Disease Activity in Juvenile Idiopathic Arthritis (JIA) [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/resilience-cumulative-social-disadvantage-and-disease-activity-in-juvenile-idiopathic-arthritis-jia/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/resilience-cumulative-social-disadvantage-and-disease-activity-in-juvenile-idiopathic-arthritis-jia/