Session Information
Session Time: 4:49PM-4:54PM
Background/Purpose: Many young adults are poorly prepared for the healthcare transition from pediatric to adult care. We identified a need for earlier and more comprehensive education about the healthcare transition in our pediatric rheumatology clinic and developed two quality improvement interventions in response.
Methods:
Since 2018, our team has tracked patients’ transition readiness using an automated, electronic health record (EHR)-based hospital-wide questionnaire (13 questions; administered annually at age ≥14 years) derived from the Got Transition Sample Transition Readiness Assessment for Youth and the Transition Readiness Assessment Questionnaire. Our goal is to improve transition readiness, measured at the population level by the proportion of questions answered “yes.”
For our first intervention, we distributed a hospital-wide, disease agnostic transition readiness education booklet in English, Spanish, and Somali to all patients aged ≥16 years at return visits to our main and satellite clinics. Booklets were distributed at the registration desk, and receipt documented by nurses in the EHR using trackable text. We solicited feedback from staff on the process.
For our second intervention, our division set a target to educate rheumatology patients aged 17-23 years and their caregivers about healthcare transition at 40% of all return visits. To meet this target, encounters required documentation of discussion of a transition/self-management topic and a goal for the patient and caregiver to work on prior to next visit. A data-enabled standard phrase with a dropdown selection of common education topics and goals was created and incorporated into clinic note templates, with the option to “write in” additional topics. Our team reviewed monthly reports of the percentage of visits successfully addressing healthcare transition.
Results:
Distribution of the booklet increased rapidly and was sustained above 50% of the target population for six months (Figure 1). Distribution then declined, perhaps indicating that many patients had already received the booklet. Throughout the study period, 765/1391 (55%) of eligible patients received a booklet at one of their clinic visits. Challenges included the lack of availability of booklets in languages other than English, Spanish, or Somali.
Education and documentation of transition topics and goals occurred at ≥54% of visits in the first month and was sustained for eight months. The most common transition topics included reviewing the transition booklet and how to communicate with the medical team (Figure 2). Throughout the study period, transition education was provided to 541/900 (60%) patients. Challenges included competing demands on time.
Patient-reported readiness to transition did not change significantly in the first six months after these interventions (Figure 3); however, as the transition readiness questionnaire is completed annually, we will require twelve months of data to fully evaluate the impact of our educational efforts.
Conclusion: Our interventions were feasible and were rapidly implemented. Further data collection is necessary to determine whether these interventions increased patients’ self-reported readiness to transition to adult care.
Transition Booklet Distribution at Visit by Clinic Site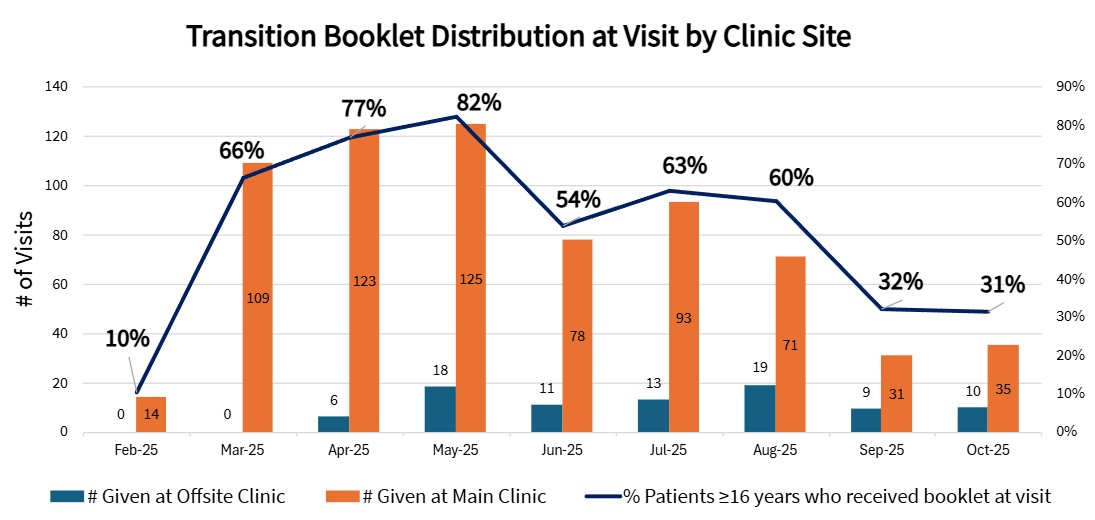 Distribution of the booklet increased rapidly and was sustained above 50% of the target population for six months. Distribution rates declined after month 6, perhaps indicating that many patients had already received the booklet.
Distribution of the booklet increased rapidly and was sustained above 50% of the target population for six months. Distribution rates declined after month 6, perhaps indicating that many patients had already received the booklet.
Documentation of Healthcare Transition Education Discussions and Goals 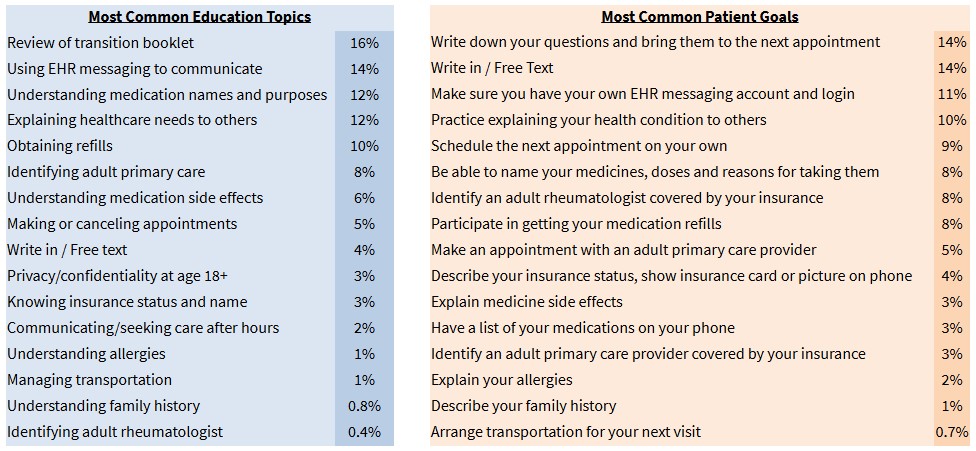 The most frequently discussed education topics and goals are listed. Beyond the suggested topics, 4% of visits included free-text “write-in” education topics such as obtaining a driver’s license, using alarms or reminders to take medications consistently, self-administering injections, and identifying a timeline for switching to an adult rheumatologist. 14% of visits included a “write in” patient goal, such as obtain guardianship, fill a pill box, save clinic phone numbers in phone contacts, attend work or school regularly, or contemplate what it would be like to transition to adult healthcare.
The most frequently discussed education topics and goals are listed. Beyond the suggested topics, 4% of visits included free-text “write-in” education topics such as obtaining a driver’s license, using alarms or reminders to take medications consistently, self-administering injections, and identifying a timeline for switching to an adult rheumatologist. 14% of visits included a “write in” patient goal, such as obtain guardianship, fill a pill box, save clinic phone numbers in phone contacts, attend work or school regularly, or contemplate what it would be like to transition to adult healthcare.
Patient-Reported Readiness to Transition to Adult Healthcare Setting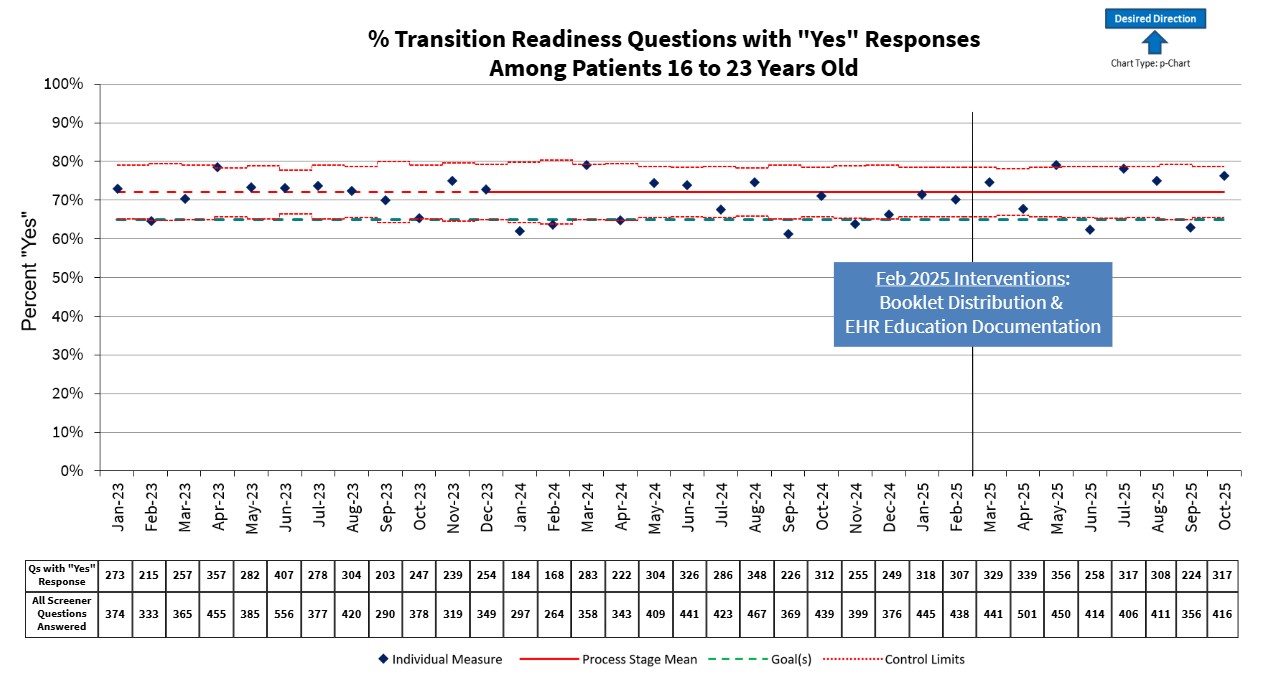 Self-reported readiness, measured by the proportion of “yes” answers to each self-management question, did not change significantly in the 12 months following the interventions. However, readiness is only assessed annually, so we expect to need an additional 6 months of follow-up to determine the impact of the interventions.
Self-reported readiness, measured by the proportion of “yes” answers to each self-management question, did not change significantly in the 12 months following the interventions. However, readiness is only assessed annually, so we expect to need an additional 6 months of follow-up to determine the impact of the interventions.
To cite this abstract in AMA style:
Murray E, Argraves M, Leone A, Taxter A, Sivaraman V, Ardoin S. Educational Interventions to Increase Transition Preparedness in a Pediatric Rheumatology Clinic [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/educational-interventions-to-increase-transition-preparedness-in-a-pediatric-rheumatology-clinic/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/educational-interventions-to-increase-transition-preparedness-in-a-pediatric-rheumatology-clinic/