Session Information
Session Time: 5:00PM-6:00PM
Background/Purpose: Structured transition programs from pediatric to adult care improve adherence to visits and treatment, patient satisfaction, quality of life, and disease-specific outcomes2. The GotTransition3 initiative provides guidance on elements of the transition process, but there has been no validated study indicating an optimal model. Current models include direct transfer to adult care, young adult clinics, adult rheumatologists joining pediatric clinic space, or shared clinic visits. At the University of Rochester Medical Center (URMC), collaboration between pediatric and adult rheumatology led to the development of a patient centered and Advanced Practice Provider (APP) led transition clinic to improve transfer of care. Here we describe our clinic model and barriers encountered in the development and implementation of this initiative.
Methods: At URMC, we created a workflow to transfer young adult patients from pediatric to adult rheumatology care using a shared visit model (“warm handoff”) in the adult rheumatology clinic space. Eligible patients were 18-22 years old, had a stable, but actively managed rheumatological disease including juvenile idiopathic arthritis, lupus, or dermatomyositis, and lived within the geographic region of our adult practice. The pediatric APP and the accepting adult APP saw patients during a one hour-long shared clinic visit that included review of clinical course, therapeutic history, expectations for adult care, and disease-specific care planning. An APP focused model was chosen to emphasize ongoing team-based care in the adult setting. Patients were assigned to an adult rheumatology attending physician for ongoing collaborative care at the time of transfer.
Results: The first transition clinics occurred in 9/2024, 12/2024, and 3/2025, but were underutilized, with only 2 successful transfers out of 12 possible appointments. Barriers identified included lack of scheduling flexibility, inadequate lead time, and conflicts with the collegiate semester schedule. Subsequent clinics occurred in 6/2025, 7/2025, 8/2025, and 10/2025 with longer lead time and more scheduling options for patients, with 14/16 possible appointments filled resulting in a successful transfer. (Table 1 and Figure 1).
Conclusion: Our APP-lead model was well accepted by patients, clinicians, and staff. Initial implementation of the clinic was limited by logistical and scheduling barriers rather than patient reluctance or unreadiness to transfer. A more patient centered approach to scheduling allowed us to increase the number of patients seen during a clinic session. Planned future steps will include more patient/family pre-clinic visit assessments of both clinical and social barriers to transition, updated formal readiness assessments, nursing engagement, and formal patient and clinician feedback.
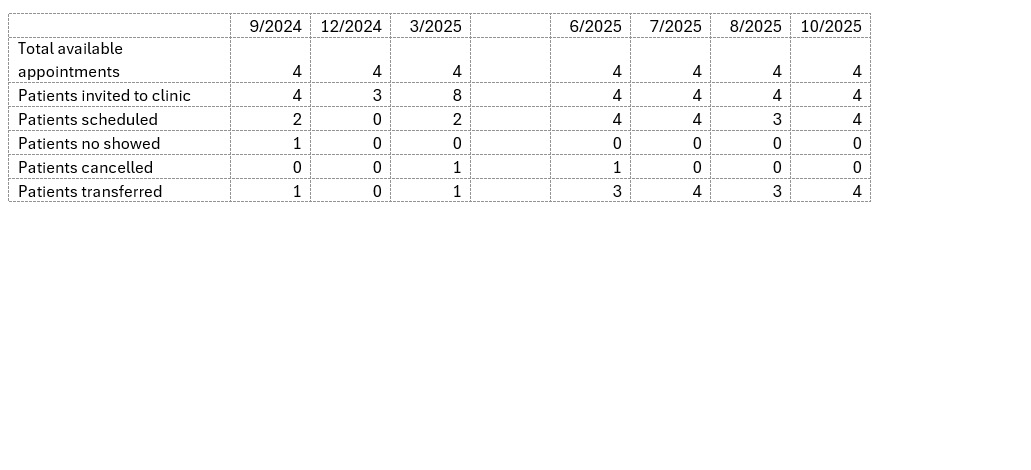 Table 1: Scheduling outcomes for pediatric to adult rheumatology transition clinics
Table 1: Scheduling outcomes for pediatric to adult rheumatology transition clinics
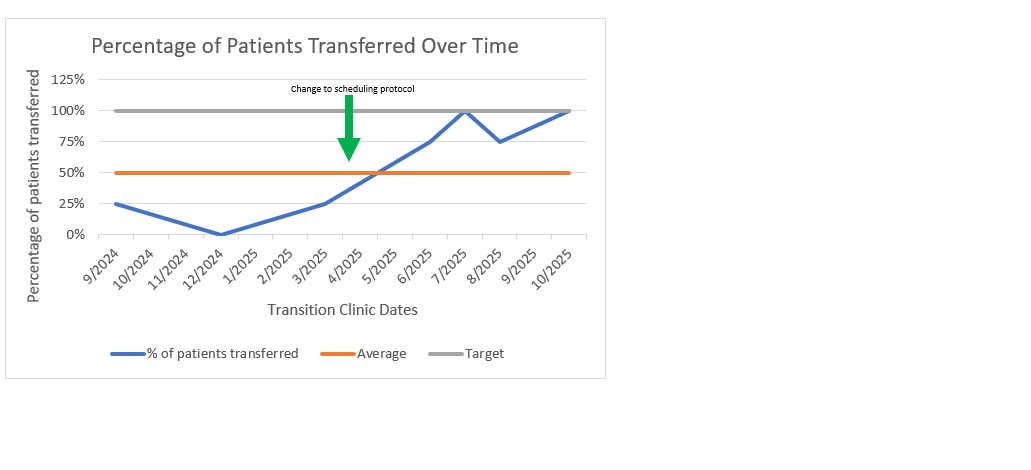 Figure 1: Percentage of patients transferred per transition clinic visit over time pre- and post- patient centered scheduling intervention
Figure 1: Percentage of patients transferred per transition clinic visit over time pre- and post- patient centered scheduling intervention
To cite this abstract in AMA style:
Pokorny C, Marston B. The Details Matter: A Patient Centered Approach to Overcoming Barriers in a Pediatric to Adult Rheumatology Transition Clinic [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/the-details-matter-a-patient-centered-approach-to-overcoming-barriers-in-a-pediatric-to-adult-rheumatology-transition-clinic/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-details-matter-a-patient-centered-approach-to-overcoming-barriers-in-a-pediatric-to-adult-rheumatology-transition-clinic/