Session Information
Session Time: 5:00PM-6:00PM
Background/Purpose: Childhood-onset systemic lupus erythematosus (cSLE) is a chronic, multisystem autoimmune disease characterized by high early disease activity and healthcare utilization. In adults, increased emergency room (ER) and hospitalization rates have been linked to disease activity, poor follow-up, and sociodemographic factors such as public health insurance and non-White race. Pediatric data remains limited. This study aimed to identify clinical and sociodemographic factors, including neighborhood opportunity (Childhood Opportunity Index, COI), associated with ER utilization among children with new-onset SLE.
Methods: A retrospective chart review of cSLE diagnosed before age 18 between January 2022 and June 2024 was done at a single, large tertiary center in southeastern United States. Data from the first year after diagnosis (included demographics, clinical features, treatment, and healthcare utilization) were summarized and compared across subgroups of COI and ER utilization. Negative binomial regression model was used to identify factors associated with ER visit frequency.
Results: Sixty patients were included: 83.3% females, 57% Hispanic; median age 15 years (IQR 13 -16). Median time from symptom onset to diagnosis was 3 months (IQR 1-6). Half had Medicaid or CHIP coverage; eight were uninsured. Major organ involvement at onset was hematologic (68%), cutaneous (58%), arthritis (55%), and renal (40%). Median SLEDAI at diagnosis was 11 (IQR 7 -17). COI mapping showed 65% lived in low/very low, 13% in moderate, and 22% in high/very high opportunity neighborhoods.
During the first year, 31 patients accounted for 61 ER visits and 36 hospitalizations. Half of ER encounters were SLE-related and 20% infection-related, most were within 3 months of diagnosis (IQR 1-6). On univariable analysis, renal disease, pleurisy, gastrointestinal involvement, higher SLEDAI, high-dose steroids and antihypertensive use were associated with increased ER visits. Kidney and gastrointestinal involvement remained significant on multivariable analysis (Table 1). Although COI was not significant overall, all four high utilizers ( >3 ER visits) lived in low-opportunity neighborhoods (Table 2). Diagnosis location, renal involvement, and SLEDAI were associated with hospitalization on univariable analysis, with renal involvement remaining significant after adjustment. No deaths were reported.
Conclusion: In this single-center cSLE cohort, renal and gastrointestinal involvement were independently associated with higher acute care utilization during the first year after diagnosis. Findings in this study highlight the impact of early disease severity on healthcare burden and the importance of identifying high-risk utilizers early to enable proactive interventions. Limitations include small sample size and single-center design. Future multicenter are needed examine how neighborhood and non-medical drivers of health further influence healthcare utilization in cSLE.
Figure 1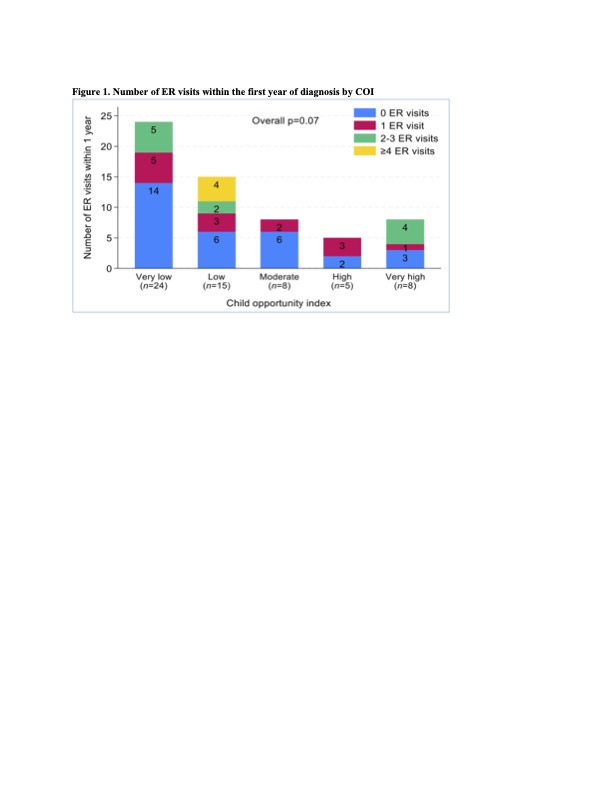 Number of ER Visits within the first year of diagnosis by COI
Number of ER Visits within the first year of diagnosis by COI
Table 1 Factors associated with ER visit number within 1 year, multivariate negative binomial regression
Factors associated with ER visit number within 1 year, multivariate negative binomial regression
Table 2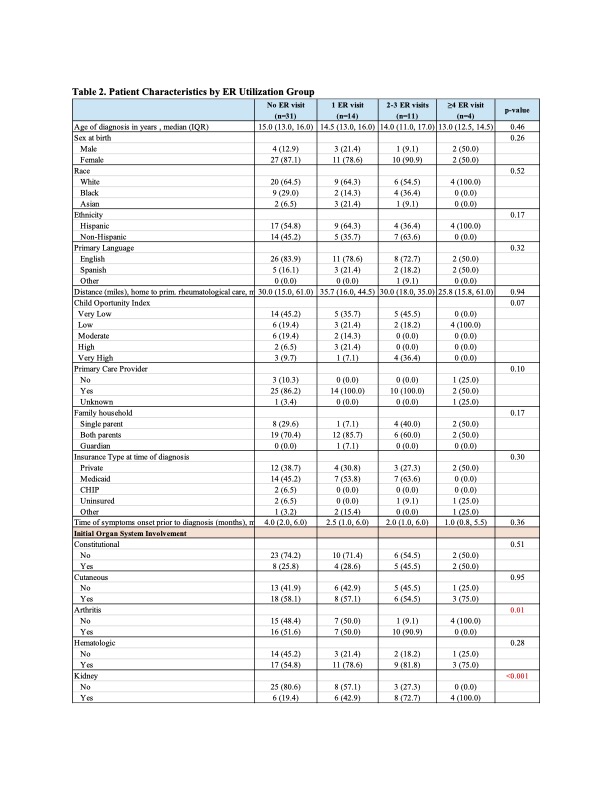 Patient Characteristics by ER Utilization Group
Patient Characteristics by ER Utilization Group
To cite this abstract in AMA style:
Miller I, Nobleza K, Nguyen D, Van Horne B, Greeley C, DeGuzman M, Thakral A, Kwan O, Molina S. Acute Care Utilization in New-Onset Childhood Systemic Lupus Erythematosus: Insights from a Pilot Study [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/acute-care-utilization-in-new-onset-childhood-systemic-lupus-erythematosus-insights-from-a-pilot-study/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/acute-care-utilization-in-new-onset-childhood-systemic-lupus-erythematosus-insights-from-a-pilot-study/