Session Information
Date: Friday, March 20, 2026
Title: Abstracts: Technology
Session Time: 4:31PM-4:36PM
Background/Purpose: Chronic nonbacterial osteomyelitis (CNO) is a rare autoinflammatory bone disease marked by heterogeneous symptoms, diagnostic delays, and variable treatment responses. It remains difficult to predict which patient will develop more severe or persistent disease. We aimed to identify subgroups of CNO patients based on longitudinal clinical trajectories and to compare their disease courses and treatment exposures.
Methods: An unsupervised machine learning (ML) clustering approach was used to identify groups of patients with similar longitudinal disease severity patterns. Patients diagnosed with CNO at ≤ 18 years of age, with ≥ 12 months of follow-up and ≥ 2 clinical visits, were included from Seattle Children’s Hospital. Longitudinal measures of disease severity, including patient pain score (0-10), clinical lesion count, patient global assessment (0-10), CDAS (clinical disease activity score to sum up 3 variables) and physician global assessment (0-10), served as inputs for clustering. After clustering, demographic and baseline features (age, sex, disease duration, lesion distribution, etc.), and medication exposures were analyzed to assess differences among the identified clusters. Chi-square tests were used for categorical variables and one-way ANOVA or Kruskal-Wallis tests for continuous variables, as appropriate. P < 0.05 was considered statistically significant.
Results: A total of 267 patients were identified. The unsupervised ML model, using multiple longitudinal severity variables, identified three patient clusters (Figure 1A). Figure 1B displays representative CDAS trajectories: persistently-low CDAS (PLC, green), progressively-improving CDAS (PIC, blue), and persistently-high CDAS (PHC, red), representing relative mild, moderate, and severe disease activity patterns. At 12 months, minimal disease activity (MDA) (CDAS ≤ 3) differed significantly among clusters, and early improvement predicted sustained control. Baseline differences (Table 1) were most evident in pain, lesion count, and global assessments (all p < 0.05). The PIC cluster (blue) had longer intervals from symptom onset to diagnosis and treatment, with the highest pain, lesion count, global assessments, ESR, and CDAS. The PLC cluster (green) remained mild, while the PHC cluster (red) showed greater inflammatory markers than PLC (green) but milder than PIC (blue), confirming a clear severity gradient. Medication exposure (Table 2) also varied: NSAID use was common (≈ 57–69%) among clusters, typically initiated within the first 6 months after diagnosis. Steroid use was higher in the PHC cluster (red), while csDMARDs, TNFi, and bisphosphonates, often started within the two years, were more frequent in the initially high-activity clusters (PIC (blue) and PHC (red)). Combination therapy increased with severity, reflecting greater treatment intensity in higher-activity clusters.
Conclusion: Unsupervised ML clustering revealed three distinct CDAS trajectories: PLC, PIC, and PHC. These findings highlight disease heterogeneity of pediatric CNO and the potential of data-driven clustering to refine prognosis, guide treatment intensity, and identify patients at risk for chronic or refractory disease.
Figure 1 Data-Driven Clustering and Longitudinal Clinical Disease Activity Score (CDAS) Patterns of Children with Chronic Nonbacterial Osteomyelitis (CNO). (Patients within the same cluster share similar longitudinal disease patterns, while those in different clusters show distinct trajectories of improvement or persistence.)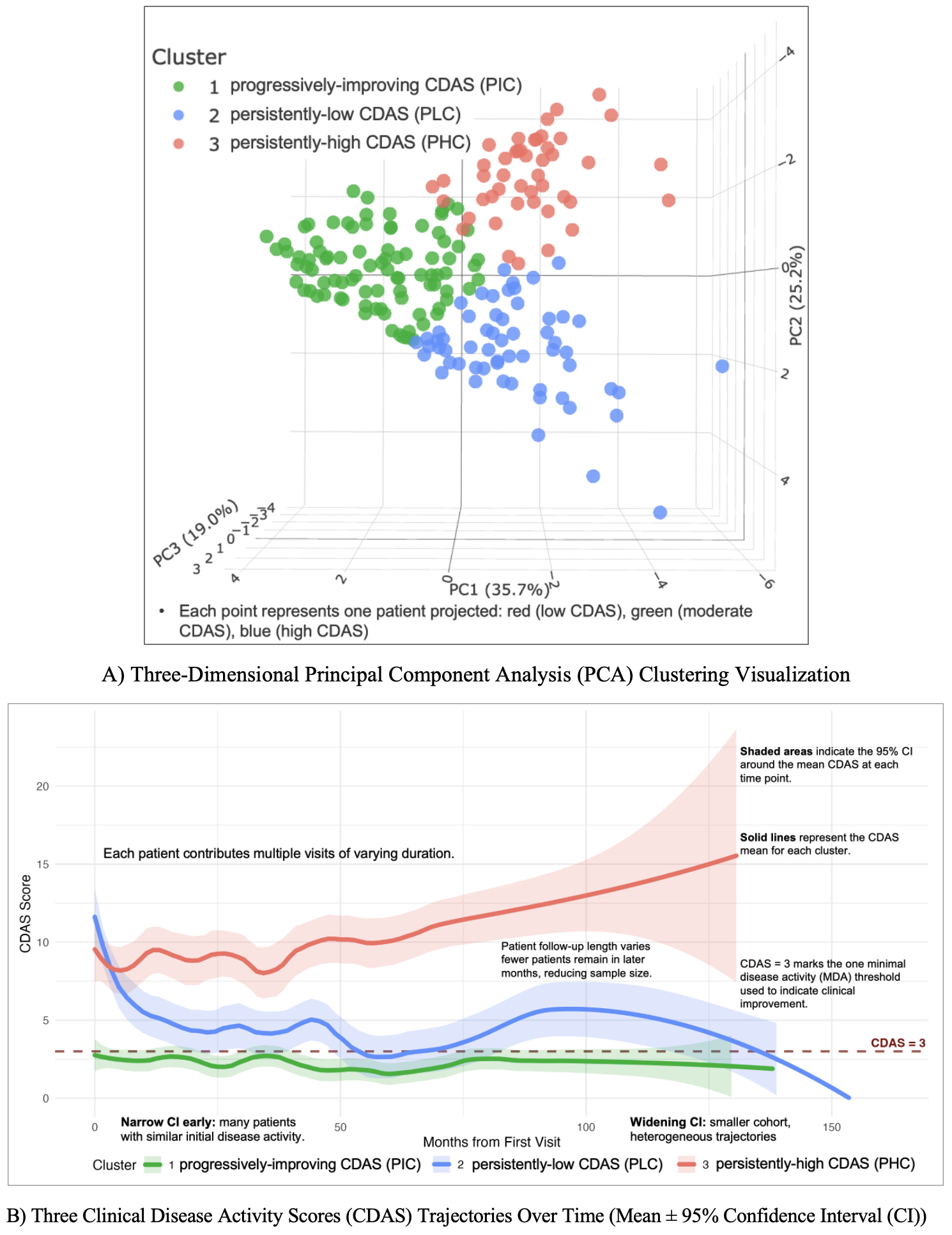 In Figure 1A: PC (principal component) is a variable that captures the maximum variance in the data along a specific direction.
In Figure 1A: PC (principal component) is a variable that captures the maximum variance in the data along a specific direction.
In Figure 1B, each patient contributes multiple visits of varying duration. Solid lines represent the CDAS mean for each cluster. Shaded areas indicate the 95% CI around the mean CDAS at each time point. Narrow CI early: many patients with similar initial disease activity. Widening CI: smaller cohort, heterogeneous trajectories
Table 1 Baseline Demographic and Clinical Characteristics Across Clusters of Disease Activity in Chronic Nonbacterial Osteomyelitis (CNO) (Data were expressed in median n (%) or mean (SD) or [IQR])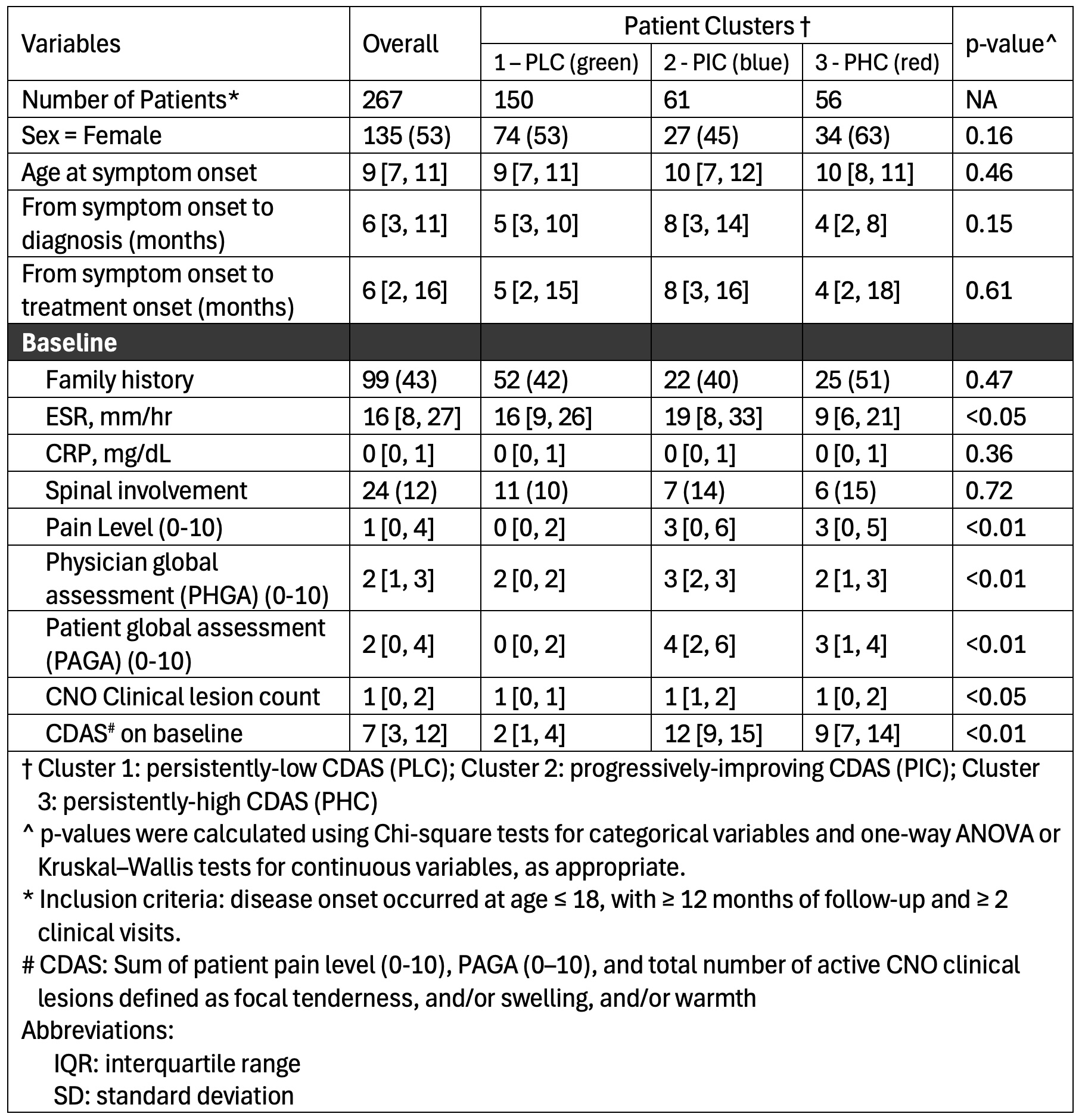 Three Clusters: Cluster 1 (persistently low CDAS, PLC) is shown in green in Figure 1; Cluster 2 (progressively improving CDAS, PIC) in blue; and Cluster 3 (persistently high CDAS, PHC) in red.
Three Clusters: Cluster 1 (persistently low CDAS, PLC) is shown in green in Figure 1; Cluster 2 (progressively improving CDAS, PIC) in blue; and Cluster 3 (persistently high CDAS, PHC) in red.
Table 2 Medication Exposure and Treatment Intensity Across Clusters of Disease Activity in Chronic Nonbacterial Osteomyelitis (CNO) (Data were expressed in median n (%) or [IQR])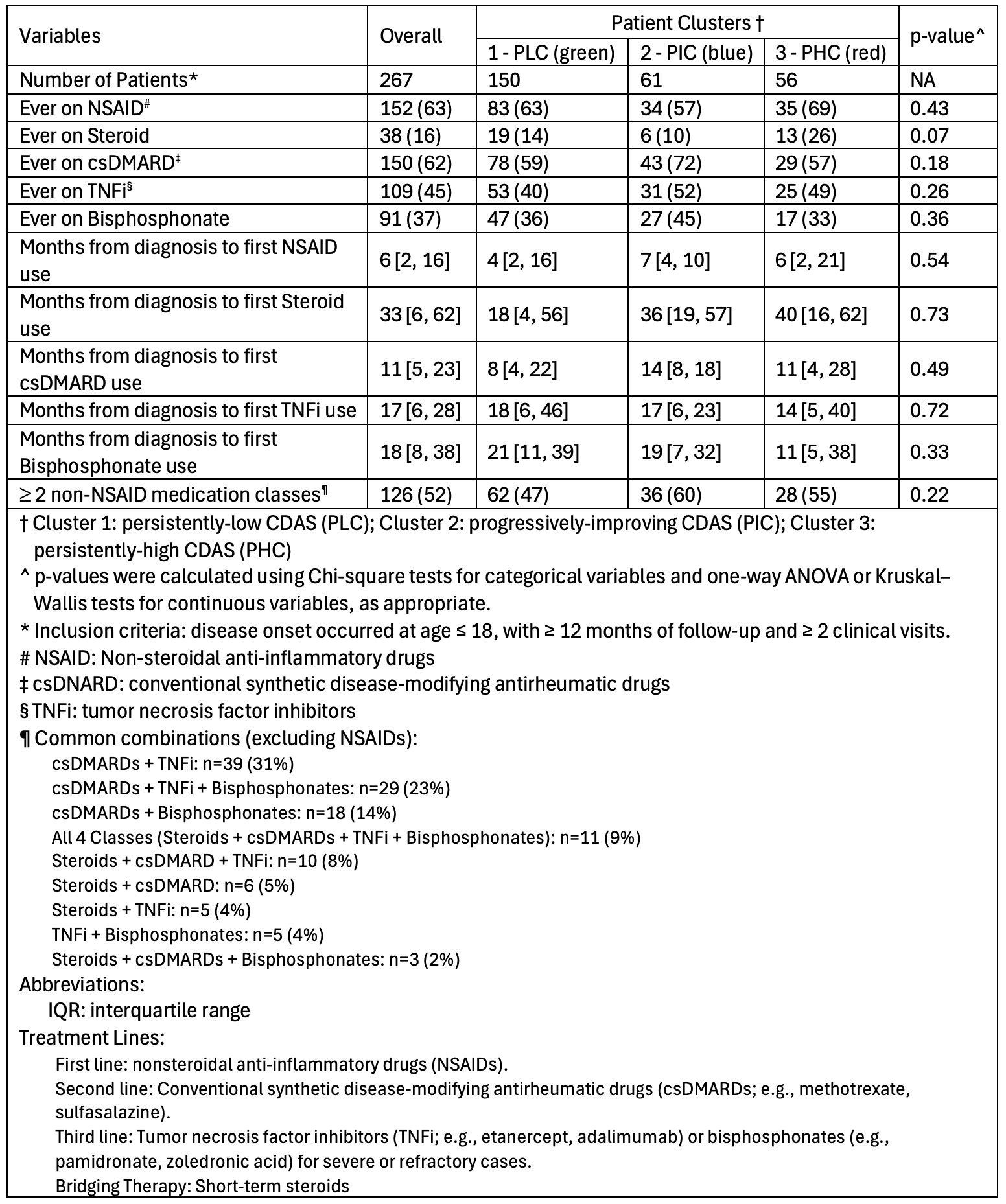 Three Clusters: Cluster 1 (persistently low CDAS, PLC) is shown in green in Figure 1; Cluster 2 (progressively improving CDAS, PIC) in blue; and Cluster 3 (persistently high CDAS, PHC) in red.
Three Clusters: Cluster 1 (persistently low CDAS, PLC) is shown in green in Figure 1; Cluster 2 (progressively improving CDAS, PIC) in blue; and Cluster 3 (persistently high CDAS, PHC) in red.
To cite this abstract in AMA style:
Chen H, Moussouras N, Wang X, Muse I, Wilson A, Nguyen M, Li Q, Wong S, Balay-Dustrude E, Rosenwasser N, Zhao Y. Identification of Distinct Disease Trajectory Patterns in Children with Chronic Nonbacterial Osteomyelitis (CNO) Using Unsupervised Machine Learning on Longitudinal Clinical Data from a Single Cohort of 267 Patients [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/identification-of-distinct-disease-trajectory-patterns-in-children-with-chronic-nonbacterial-osteomyelitis-cno-using-unsupervised-machine-learning-on-longitudinal-clinical-data-from-a-single-cohort/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/identification-of-distinct-disease-trajectory-patterns-in-children-with-chronic-nonbacterial-osteomyelitis-cno-using-unsupervised-machine-learning-on-longitudinal-clinical-data-from-a-single-cohort/