Session Information
Session Time: 5:00PM-6:00PM
Background/Purpose: Juvenile localized scleroderma (jLS) is a chronic autoimmune, fibrosing condition associated with a high burden of damage, including functional impairment. Severe morbidity most often results from extracutaneous involvement (ECI), with musculoskeletal complications being the most common. Among these, growth differences (GD)—such as limb-length discrepancies or craniofacial hemiatrophy—are particularly consequential, affecting a child’s development, function, and appearance. Despite their clinical significance, the development and characteristics of GD in jLS have been infrequently studied. The objective of this study was to characterize the pattern of GD and identify features associated with their presence in a single-center jLS cohort.
Methods: A retrospective chart review was conducted of consecutive patients with JLS who were seen at Hackensack University Medical Center between 6/2018-2/2025. Collected data included demographics, disease pattern, autoantibody profiles, and family history. Craniofacial and truncal GD were defined as presence of an obvious asymmetry in major structures (e.g., eye, nose, breast) based on clinical assessment (SCL), imaging (MRI, X-ray, or ultrasound), and/or measurements. Limb GD included limb girth and limb length differences, and were defined as at least a 0.5 cm difference between affected and unaffected regions, or imaging identified differences in volume. Differences between groups were evaluated by Fisher’s exact test (categorical variables ) or Mann-Whitney test (continuous variables).
Results: Fifty-two patients were included, of whom 44 (84.6%) had ECI and 30 (57.7%) a GD (Table). Patients with GD were diagnosed at a younger age than those without GD (median 7.1 [IQR 5.1–11.2] vs. 12.8 [IQR 8.9–15.4] years, P = 0.016). Groups did not differ with respect to sex or time to diagnosis. GD was associated with the linear scleroderma subtype (p = 0.049) and with extremity involvement (p = 0.005). Patients with truncal involvement were less likely to develop a GD (p < 0.001), while craniofacial involvement was not found to influence GD development . Among individuals with extremity disease, 23 (74%) developed a girth difference and 13 (42%) a limb-length discrepancy. Nine patients (30%) had GD affecting multiple anatomic regions, most commonly the trunk and an extremity (Figure 2). GD was already present at diagnosis in 11 patients (36.7%). These individuals did not differ from the overall GD cohort in age at diagnosis or time to diagnosis. Of these early-identified GD cases, five involved the craniofacial region, three involved an extremity, and three involved both the trunk and an extremity
Conclusion: In our jLS cohort, more than half of the children exhibited a growth difference (GD), with 30% of them having involvement of multiple anatomic regions. GDs were associated with the linear scleroderma subtype, autoantibody positivity, and a younger age at LS diagnosis. Approximately one-third of affected patients already demonstrated GD at the time of diagnosis. These findings underscore the need for further research to better understand, detect, and improve outcomes for this common and severe morbidity.
Table: Characteristics of JLS patients with and without Growth Differences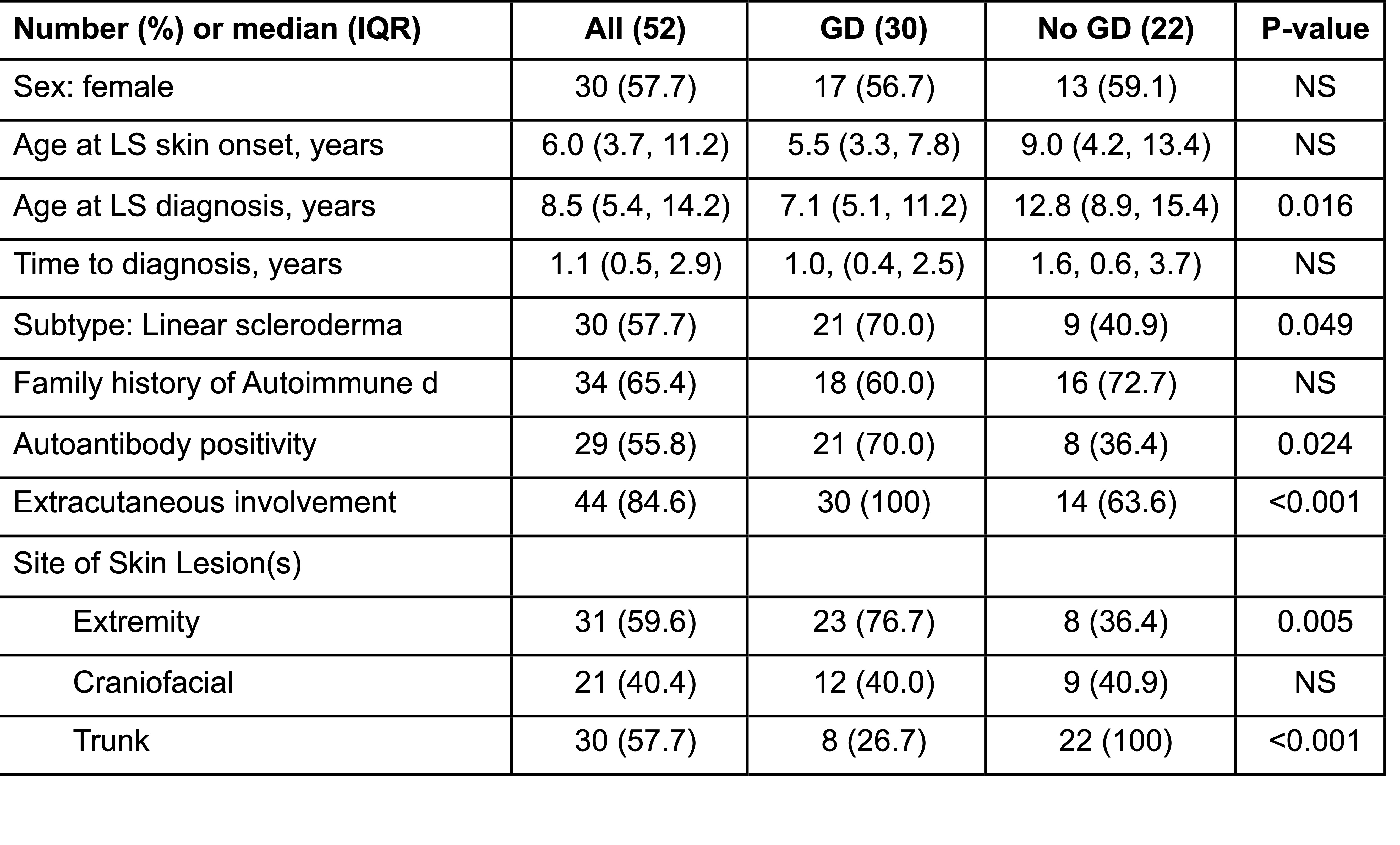 The disease patterns of the whole cohort and of the jLS patients who had and did not have a growth difference (GD) are shown. GD were associated with the linear subtype, having skin lesion(s) on an extremity, autoantibody positivity, and a younger age at LS diagnosis. GD were less commonly found in patients who had truncal involvement. Differences between the patients with and without a GD were calculated by Fisher’s exact test or Mann-Whitney test.
The disease patterns of the whole cohort and of the jLS patients who had and did not have a growth difference (GD) are shown. GD were associated with the linear subtype, having skin lesion(s) on an extremity, autoantibody positivity, and a younger age at LS diagnosis. GD were less commonly found in patients who had truncal involvement. Differences between the patients with and without a GD were calculated by Fisher’s exact test or Mann-Whitney test.
Figure 1: Frequency of Growth Difference Development for each Anatomic Region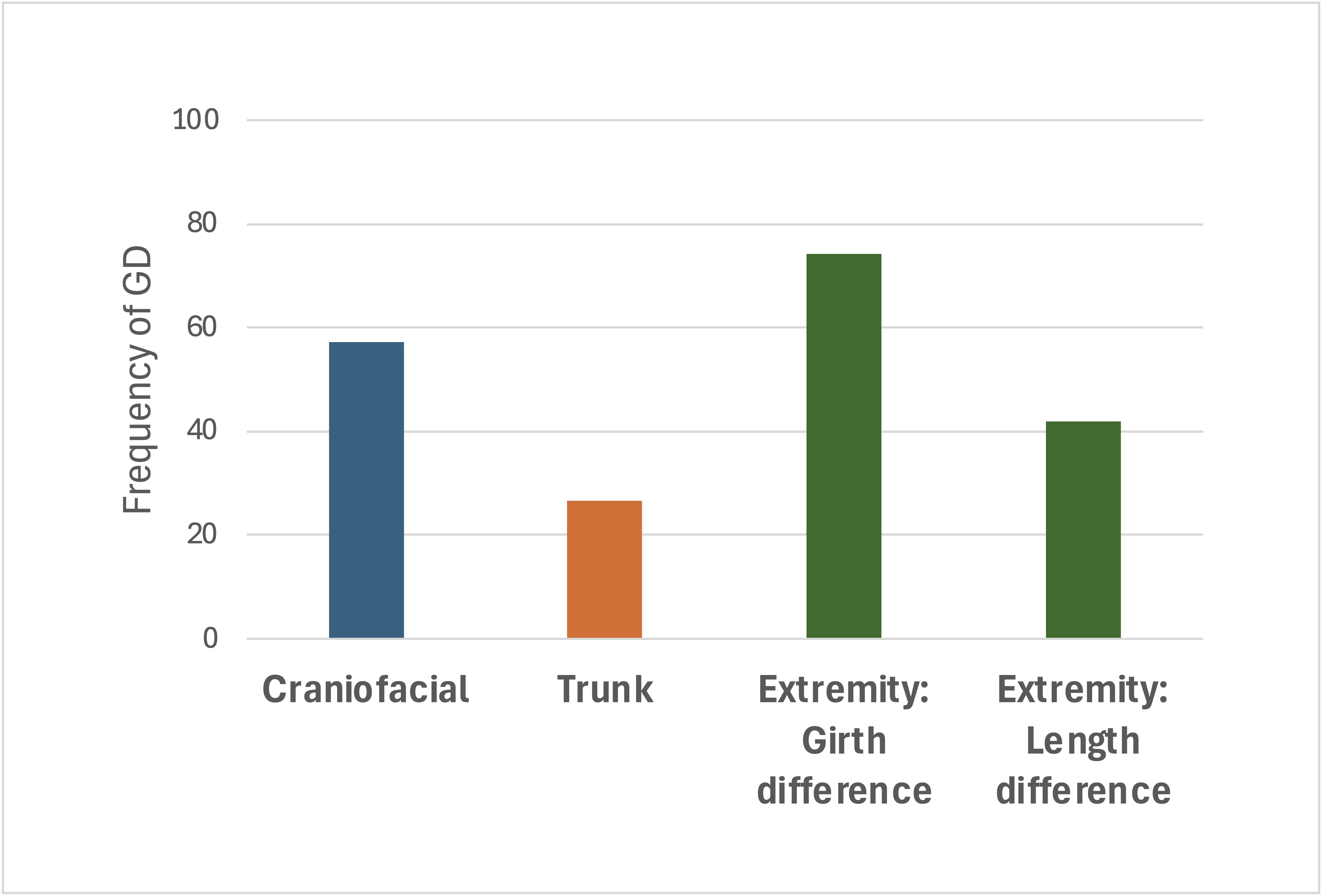 The percent of patients that developed a growth difference (GD) for each skin involvement region is shown. About half the patients that had craniofacial skin involvement developed a GD (12/21, 57%). Most of the patients that had skin involvement of an extremity developed a GD (23/31, 74%), compared to a minority of the patients that had skin involvement of the trunk (8/30, 27%).
The percent of patients that developed a growth difference (GD) for each skin involvement region is shown. About half the patients that had craniofacial skin involvement developed a GD (12/21, 57%). Most of the patients that had skin involvement of an extremity developed a GD (23/31, 74%), compared to a minority of the patients that had skin involvement of the trunk (8/30, 27%).
Figure 2: Pattern of Growth Difference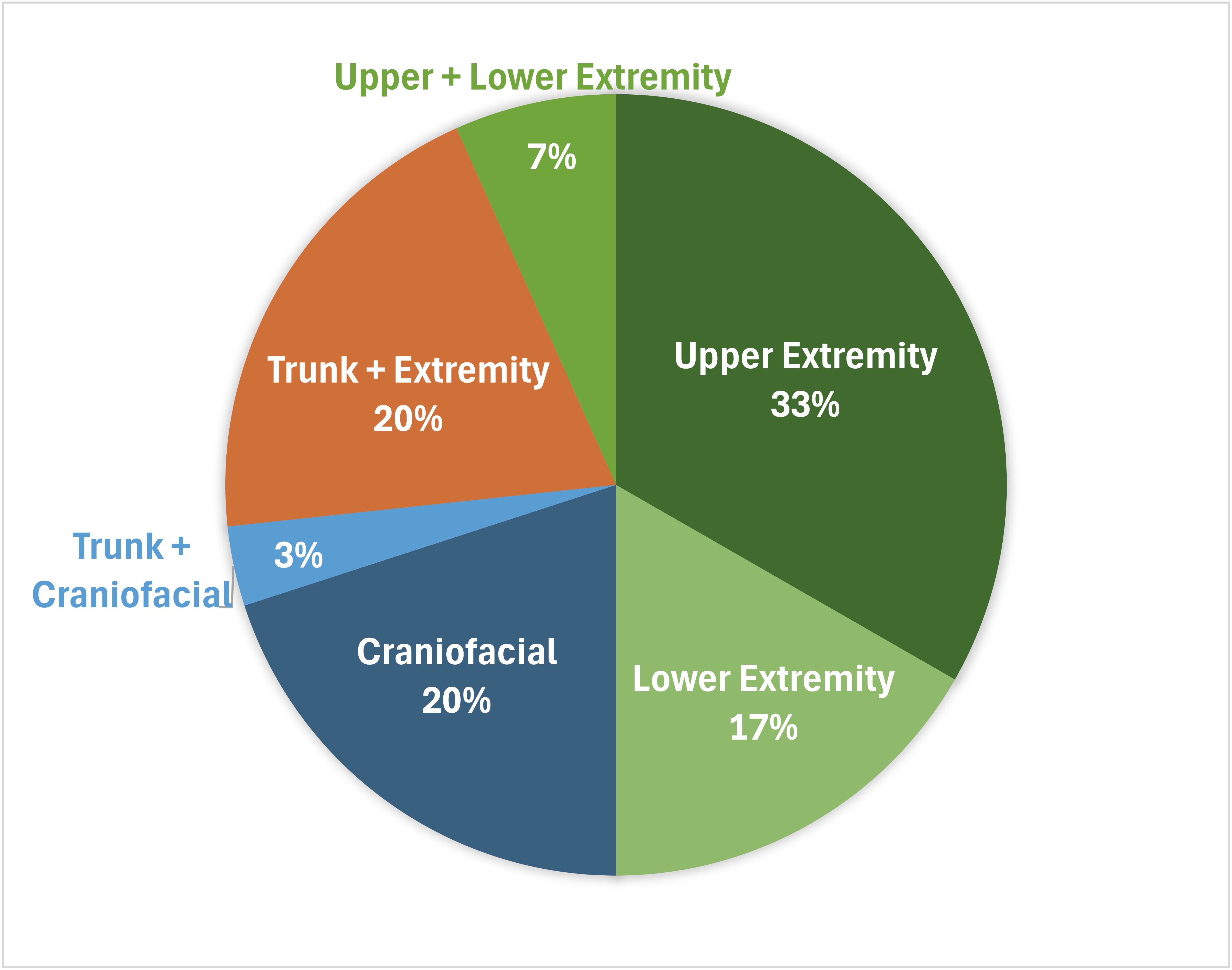 The location of the growth differences (GD) identified in the 30 jLS patients with a GD are shown. The upper extremity was the most commonly affected site (33%). Thirty percent of the patients had multiple anatomic regions affected, most commonly the trunk and an extremity (20%).
The location of the growth differences (GD) identified in the 30 jLS patients with a GD are shown. The upper extremity was the most commonly affected site (33%). Thirty percent of the patients had multiple anatomic regions affected, most commonly the trunk and an extremity (20%).
To cite this abstract in AMA style:
Paek B, Li S. A Growing Problem: Factors Associated with Growth Disturbances in Juvenile Localized Scleroderma [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/a-growing-problem-factors-associated-with-growth-disturbances-in-juvenile-localized-scleroderma/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-growing-problem-factors-associated-with-growth-disturbances-in-juvenile-localized-scleroderma/