Session Information
Session Time: 5:00PM-6:00PM
Background/Purpose: Intra-articular glucocorticoids (IAGCs) are a common first-line therapy for patients with oligoarticular juvenile arthritis. Limited data exist on rates and predictors of treatment escalation following initial IAGC use.
Avramovic et al. (2024) reported that 46% of patients treated with IAGC initially required systemic therapy. Younger age, ANA positivity, and HLA-B27 presence were predictive factors for systemic therapy use.
This study aimed to determine the percentage of patients requiring systemic therapy within 6 and 12 months of diagnosis after receiving IAGCs as initial treatment and to identify clinical factors associated with treatment escalation.
Methods: We conducted a single-center retrospective review of patients with JIA initially treated with IAGCs only. Patients with uveitis were excluded. Systemic therapy was defined as the use of either conventional or biologic disease-modifying antirheumatic drug. Statistical analysis included Fisher’s exact and Chi-square tests.
Results: Ninety-two patients met inclusion criteria (Table 1).
Overall, 33% required systemic therapy within 6 months and 46% required systemic therapy within 12 months.
Age ≤ 6 years at diagnosis was not significantly associated with risk of systemic therapy at either timepoint.
Patients presenting with 3–5 joints were significantly more likely to require systemic therapy at 6 months and 12 months than those presenting with 1–2 joints.
Use of triamcinolone acetonide for the initial procedure was associated with higher rates of systemic therapy initiation at both timepoints compared with triamcinolone hexacetonide.
ANA positivity did not predict systemic therapy at 6 months but became significant at 12 months (Table 2).
Among patients with early-onset arthritis and 1-2 joints treated with triamcinolone hexacetonide, ANA status did not significantly influence the need for systemic therapy at either timepoint (Table 3).
Conclusion: In this cohort, 33% and 46% of patients required systemic therapy within 6 months and 12 months from diagnosis, respectively.
Two factors emerged as predictors of treatment escalation: involvement of 3-5 joints at diagnosis and use of triamcinolone acetonide rather than triamcinolone hexacetonide. This suggests that a presentation at the higher end of the oligoarticular range could indicate either a more aggressive phenotype with reduced likelihood of remission from local therapy alone or increased likelihood of IAGC refractory joints.
While ANA positivity was not associated with systemic therapy at 6 months, it became a statistically significant predictor for requirement of systemic therapy by 12 months. Among patients with 1-2 joints, ANA status showed a trend toward higher risk at both timepoints, though not statistically significant. The results of this study may help guide decision-making for clinicians managing new onset oligoarticular JIA. IAGCs are likely to be more successful in patients with 1-2 joints involved, negative ANA status, and when triamcinolone hexacetonide is available.
Table 1. Patient Demographics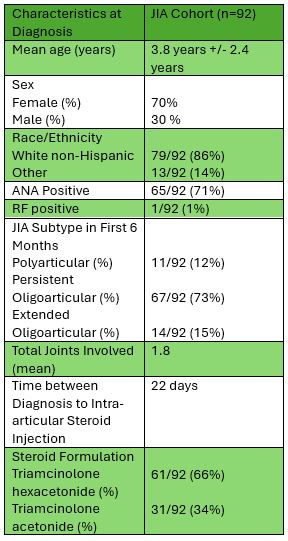
Table 2. Results 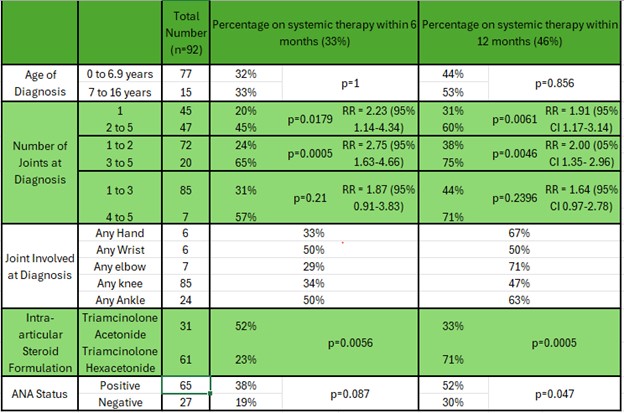
Table 3. Early Onset Arthritis Analysis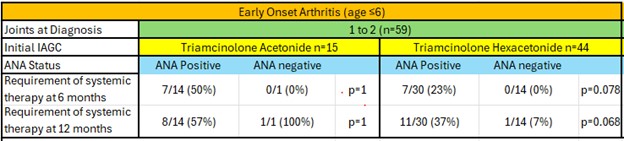
To cite this abstract in AMA style:
Kung A, Hays K, Scalzi L, Bingham C, Yu Asensi F, Hahn T. Outcomes of Oligoarticular Juvenile Idiopathic Arthritis Patients Treated with Intra-articular Glucocorticoids: Can We Predict Successful Treatment? [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/outcomes-of-oligoarticular-juvenile-idiopathic-arthritis-patients-treated-with-intra-articular-glucocorticoids-can-we-predict-successful-treatment/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/outcomes-of-oligoarticular-juvenile-idiopathic-arthritis-patients-treated-with-intra-articular-glucocorticoids-can-we-predict-successful-treatment/