Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose: 5-10% of patients with juvenile idiopathic arthritis (JIA) can have chronic pain lasting >3 months despite well-controlled disease. This pain is from altered pain-related sensory pathways in the periphery and central nervous system, causing increased sensitivity. Chronic pain despite resolution of inflammation can lead to poorer quality of life, psychological distress, and increased healthcare seeking. Therefore, we should address chronic pain during treatment of JIA. Our aim is to deliver standardized chronic pain education to 50% of patients with JIA who meet predefined thresholds for chronic pain over 6 months using quality improvement (QI) methodology.
Methods:
Using Plan-Do-Study-Act (PDSA) cycles, the following change ideas were completed: (1) Creation of an institution-specific handout explaining pain and options for treatment. This involved iterative review by faculty and fellows in the Divisions of Rheumatology and Pain Medicine, as well as a patient, parents, and Seattle Children’s education team. (2) Lecture to division on definition of chronic pain, thresholds at which to consider diagnosis, and treatments, which was reinforced in monthly meetings. (3) Creation of electronic medical record order set to standardize ICD-10 coding for chronic pain, use pre-filled orders, and efficiently print the handout in clinic.
The cohort included patients with JIA ≥ 8 years old from a quaternary outpatient center. Those with a pain score of ≥ 4 (scale 0-10) and discrepancy between patient and physician global assessment scores of ≥ +30 (scale 0-100) met inclusion criteria. These scores are routinely documented at clinic visits. Patients with missing scores were excluded.
The numbers of patients who did and did not receive the chronic pain education handout (based on physician documentation) were extracted from electronic health records per month between June to September 2025.
Results: The handout is now available online. Per month, an average of 117 patients were seen, 4-7 met inclusion criteria, and an additional 1-7 had a preexisting diagnosis of chronic pain. Following four months of three PDSA cycles, our 50% target was met (Table 1).
Conclusion: We established and implemented a framework to diagnose and educate patients with JIA and chronic pain, meeting our goal of reaching 50% of patients with chronic pain. The next steps are to determine the sustainability of this and identify barriers. Future directions include assessment of balancing measures and physician and patient satisfaction with this education initiative. Limitations include inaccurate documentation, such as if the handout was provided but not documented, and missing pain/global scores. This represents our first step towards optimizing long-term pain outcomes in children with JIA.
Figure 1: Screenshot of first page of handout Available at https://www.seattlechildrens.org/globalassets/documents/for-patients-and-families/pfe/pe4226.pdf or by accessing QR code.
Available at https://www.seattlechildrens.org/globalassets/documents/for-patients-and-families/pfe/pe4226.pdf or by accessing QR code.
Figure 2: Key driver diagram (KDD) 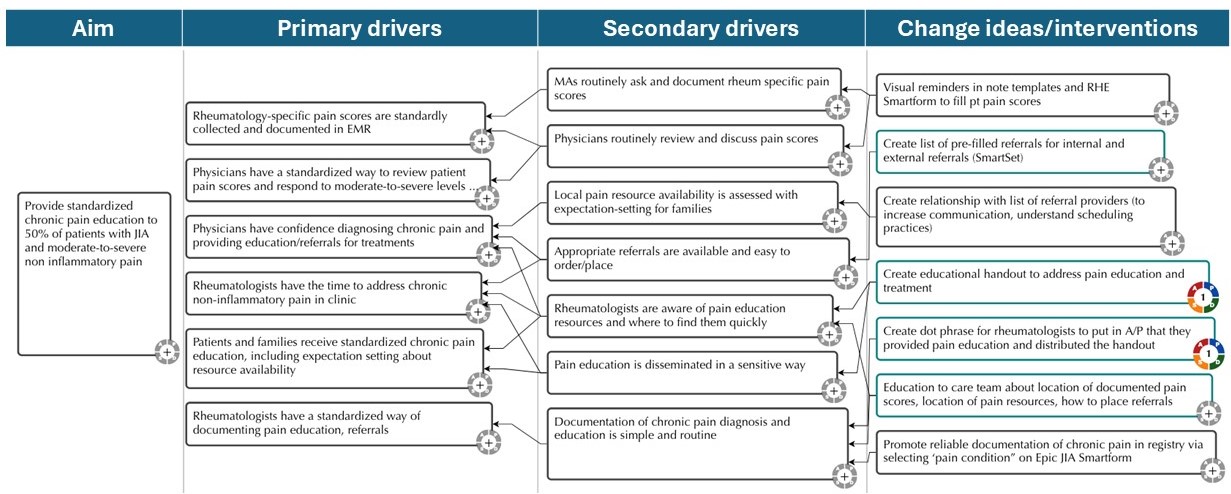 Key driver diagram (KDD) that presents the primary drivers, secondary drivers, and change ideas for delivering standardized education to patients with JIA and moderate-to-severe non-inflammatory chronic pain in an outpatient pediatric rheumatology clinic. Change ideas/interventions in teal boxes were implemented in this abstract.
Key driver diagram (KDD) that presents the primary drivers, secondary drivers, and change ideas for delivering standardized education to patients with JIA and moderate-to-severe non-inflammatory chronic pain in an outpatient pediatric rheumatology clinic. Change ideas/interventions in teal boxes were implemented in this abstract.
Table 1: Primary and secondary outcome measures 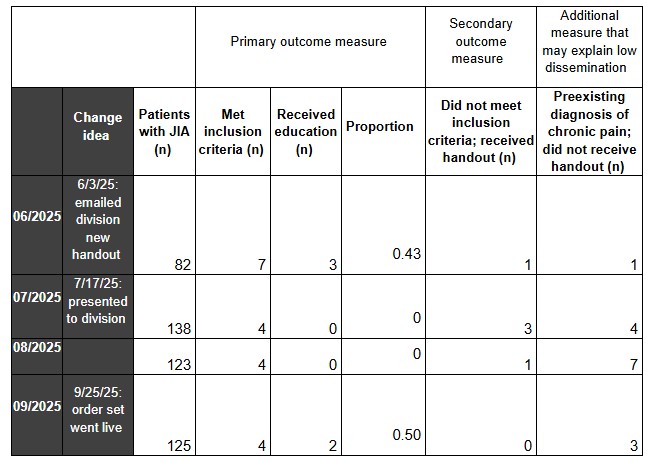 Numbers in table represent number of patients, unless otherwise specified. Outcome measures, including primary outcome (proportion of patients who received the chronic pain education handout out of those who met inclusion criteria), secondary outcome (patients with JIA who did not meet thresholds but still received educational materials according to the physician’s attestation), and number of patients who had likely already received some chronic pain education and treatment from a rheumatologist in the past and thus did not receive handout during observation period. Data presented by calendar month across our three outpatient rheumatology clinics. JIA = juvenile idiopathic arthritis.
Numbers in table represent number of patients, unless otherwise specified. Outcome measures, including primary outcome (proportion of patients who received the chronic pain education handout out of those who met inclusion criteria), secondary outcome (patients with JIA who did not meet thresholds but still received educational materials according to the physician’s attestation), and number of patients who had likely already received some chronic pain education and treatment from a rheumatologist in the past and thus did not receive handout during observation period. Data presented by calendar month across our three outpatient rheumatology clinics. JIA = juvenile idiopathic arthritis.
To cite this abstract in AMA style:
Ferguson R, Radford L, Friedrichsen E, Tham S, Morgan E, Rosenwasser N. Standardizing Effective Education and Intervention for Chronic Non-Inflammatory Pain in Children with Juvenile Idiopathic Arthritis: A Quality Improvement Initiative [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/standardizing-effective-education-and-intervention-for-chronic-non-inflammatory-pain-in-children-with-juvenile-idiopathic-arthritis-a-quality-improvement-initiative/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/standardizing-effective-education-and-intervention-for-chronic-non-inflammatory-pain-in-children-with-juvenile-idiopathic-arthritis-a-quality-improvement-initiative/