Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose: Autoimmune diseases frequently affect adolescents and young adults (AYAs) of childbearing age. In a recent study, 36% of AYAs in rheumatology clinics reported using teratogenic medications, yet only half of these patients received reproductive counseling and pregnancy screening (Huynh, B., Ott, M.A., Tarvin, S.E, Pediatr Rheumatol 23, 5 2025). Most preferred to receive such counseling from rheumatology rather than primary care providers, highlighting the need for stronger reproductive health counseling and screening in rheumatology clinics. We aim to increase reproductive health counseling and screening by 30% among patients of reproductive age (11–23 years, post-menarche) receiving teratogenic medications in the pediatric rheumatology clinic by June 2026 through collaboration with diverse stakeholders.
Methods:
A multidisciplinary team of clinicians, nurses, pharmacists, trainees, social workers, patient and parent representatives, and community representatives met monthly to design and implement this quality improvement (QI) project at Albany Medical Center Pediatric Rheumatology Clinic. A chart review of 32 patients on teratogenic medications established baseline counseling and screening rates. Progress will be tracked via chart reviews (n=32 per PDSA cycle) using iterative interventions. A Key Driver Diagram (Figure 1) identified key targets: (a) provider education, (b) pregnancy screening, (c) counseling for patients and parents, (d) documentation of sexual history, and (e) patient satisfaction. Initial interventions included an in-service training on teratogenic medications and best practices per the 2020 ACR Reproductive Health Guidelines, with pre- and post-surveys to assess knowledge gain. A new smart phrase was created and shared to improve EMR documentation and detection. In addition, subsequent and ongoing interventions are listed in the key driver diagram. QI tools include PDSA worksheets, flowcharts, run charts, and control charts.
Results:
Baseline review showed only 1 of 32 patients (3%) had documented sexual health counseling in the past six months. Two (6%) received pregnancy screening, 18 (56%) had no documented screening, and 12 (38%) were male and not eligible. In-service training improved provider knowledge scores by 10%, and afterward, 100% rated discussing reproductive health with AYAs as “extremely important.” Preliminary results of PDSA cycle 1 show a 30% increase in documented counseling (n=24) and 19% increase in screening (n=14). Barriers identified by providers include time constraints, forgetting counseling, and hesitancy to initiate discussions on what could be perceived as ‘taboo topics’ for some patients and parents.
Conclusion: Through stakeholder engagement and QI methodology, this project aims to enhance reproductive health counseling and screening for AYAs on teratogenic medications in pediatric rheumatology. Other ongoing interventions include pre-visit planning to identify eligible patients, a Quick Reference Sheet in all exam rooms, and standard provider verbiage training by parent and community representatives.
Key Driver Diagram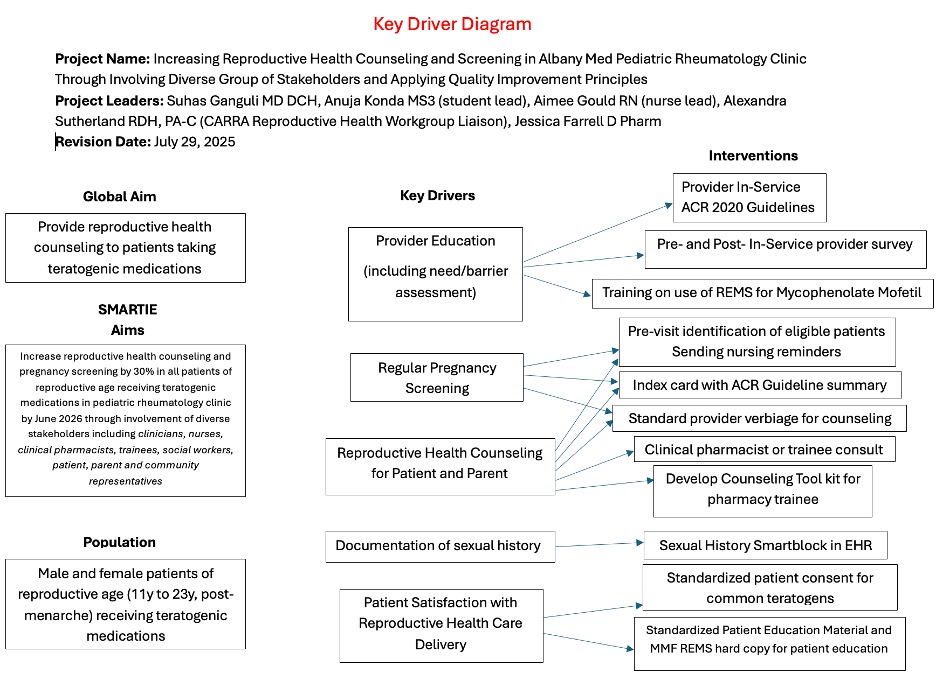
Comparison of Providers’ Scores Pre and Post In-service Knowledge Levels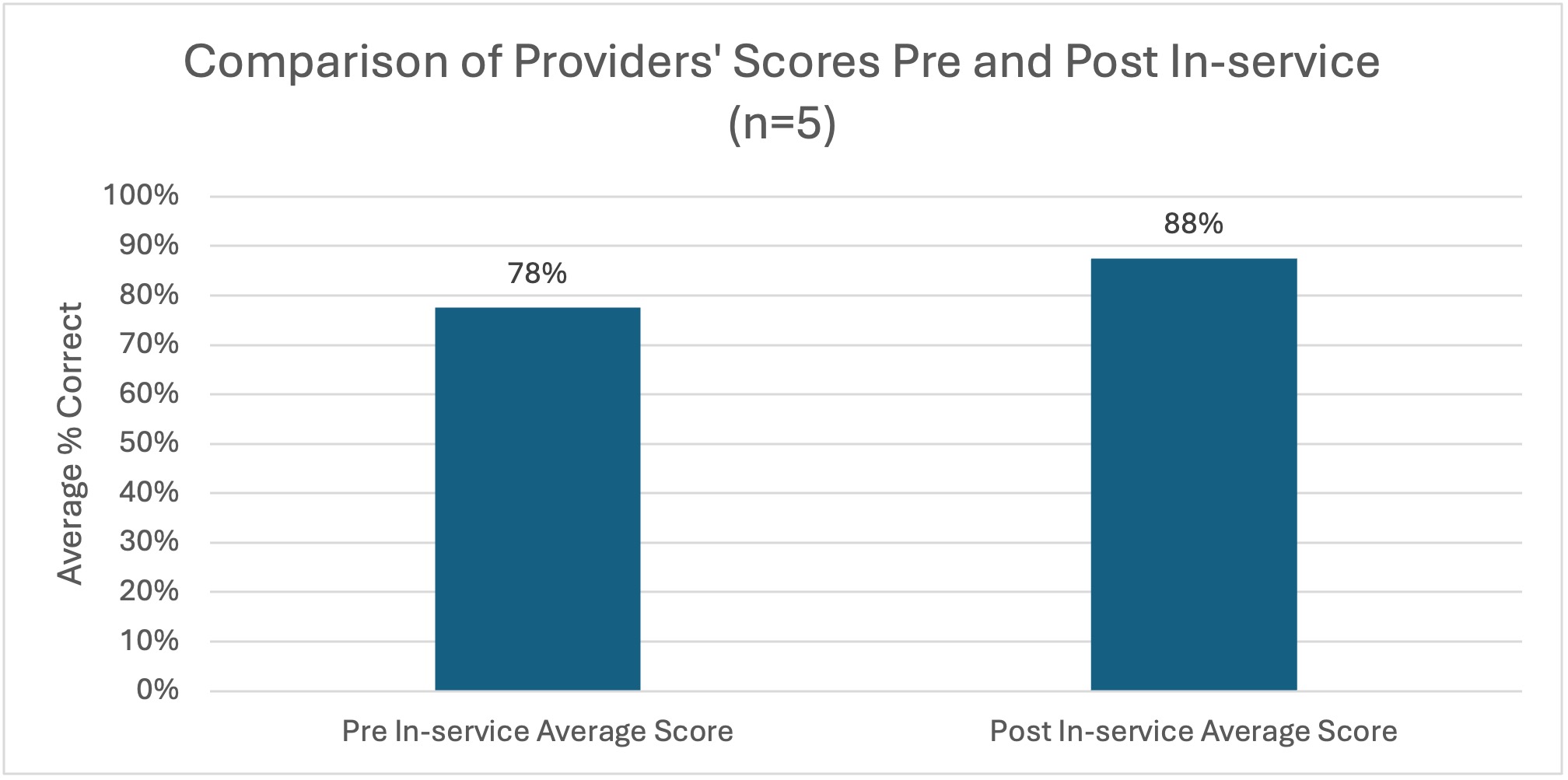
Current and Select Future PDSA Cycles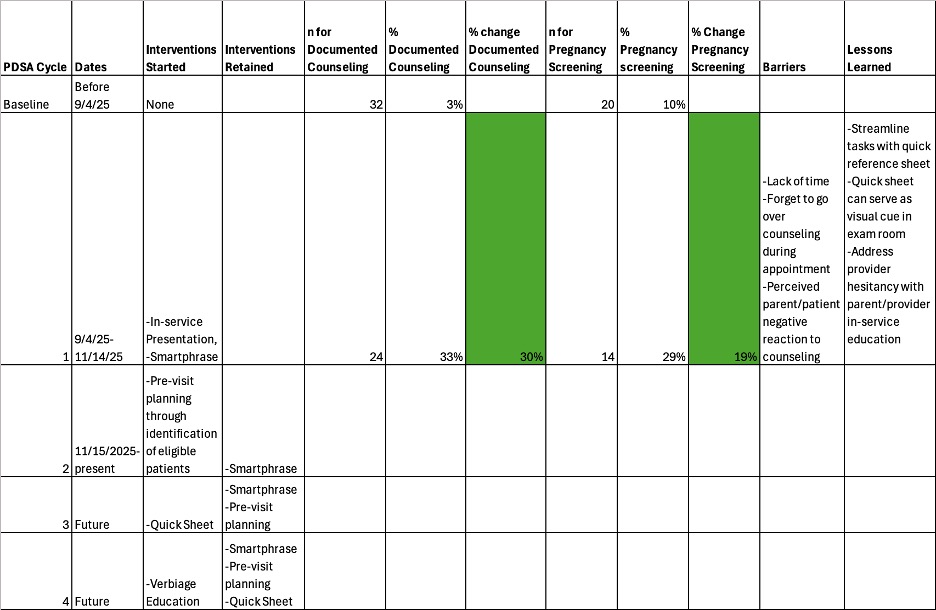
To cite this abstract in AMA style:
Konda A, Farrell J, Hughes K, Gould A, Sutherland A, Ostrov B, Bermudez-Santiago L, Salvant C, Doemel R, Ganguli S. Increasing Reproductive Health Counseling and Screening in a Pediatric Rheumatology Clinic Using Quality Improvement Principles and Diverse Group of Stakeholders [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/increasing-reproductive-health-counseling-and-screening-in-a-pediatric-rheumatology-clinic-using-quality-improvement-principles-and-diverse-group-of-stakeholders/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/increasing-reproductive-health-counseling-and-screening-in-a-pediatric-rheumatology-clinic-using-quality-improvement-principles-and-diverse-group-of-stakeholders/