Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose: Systemic juvenile idiopathic arthritis-associated lung disease (sJIA-LD) is a rare, potentially fatal complication of sJIA, often accompanied by pulmonary hypertension (PH) and macrophage activation syndrome (MAS). The underlying pathophysiology remains poorly understood and optimal management strategies have yet to be established. Recent retrospective data suggests that combination therapy with cyclophosphamide (CYC) and rituximab (RTX) may be both safe and effective in children with severe or life-threatening manifestations of rheumatic disease. However, literature on CYC-RTX use in sJIA-LD is lacking.
Methods: We describe two pediatric cases of sJIA-LD complicated by PH and recurrent episodes of MAS. Both patients remained refractory to conventional sJIA therapies, necessitating escalation with combination CYC-RTX.
Results: Following combination CYC–RTX therapy, both patients demonstrated marked clinical improvement, including resolution of hyperferritinemia, normalization of acute phase reactants, and recovery of hepatic function profiles. Patient 1 experienced a reduction in outpatient supplemental oxygen requirement from 1 liter per minute continuously to 0.5 liter per minute nocturnally. Patient 2 experienced a resolution of growth failure with initial length significantly less than the 3rd percentile and final height greater than the 10th percentile. Chest computed tomography showed notable improvements in bronchiectasis, ground-glass opacities, and septal and pleural thickening in both patients. Patient 1 exhibited significant improvement in pulmonary hypertension on right heart catheterization, with mean pulmonary arterial pressure decreasing from 47 to 25 mmHg and pulmonary vascular resistance decreasing from 11.1 to 4.3 Wood units, while pulmonary capillary wedge pressure remained normal. Both patients were also able to substantially reduce their daily prednisone requirements following combination therapy: from 1 mg/kg/day to < 0.2 mg/kg/day in patient 1, and complete discontinuation in patient 2, who had previously been on 2 mg/kg/day.
Conclusion: Combination therapy with CYC and RTX may represent a valuable therapeutic approach in refractory sJIA complicated by lung disease, particularly in patients with concomitant MAS or PH.
Case 1 sJIA-LD Disease Activity Biomarkers Over Time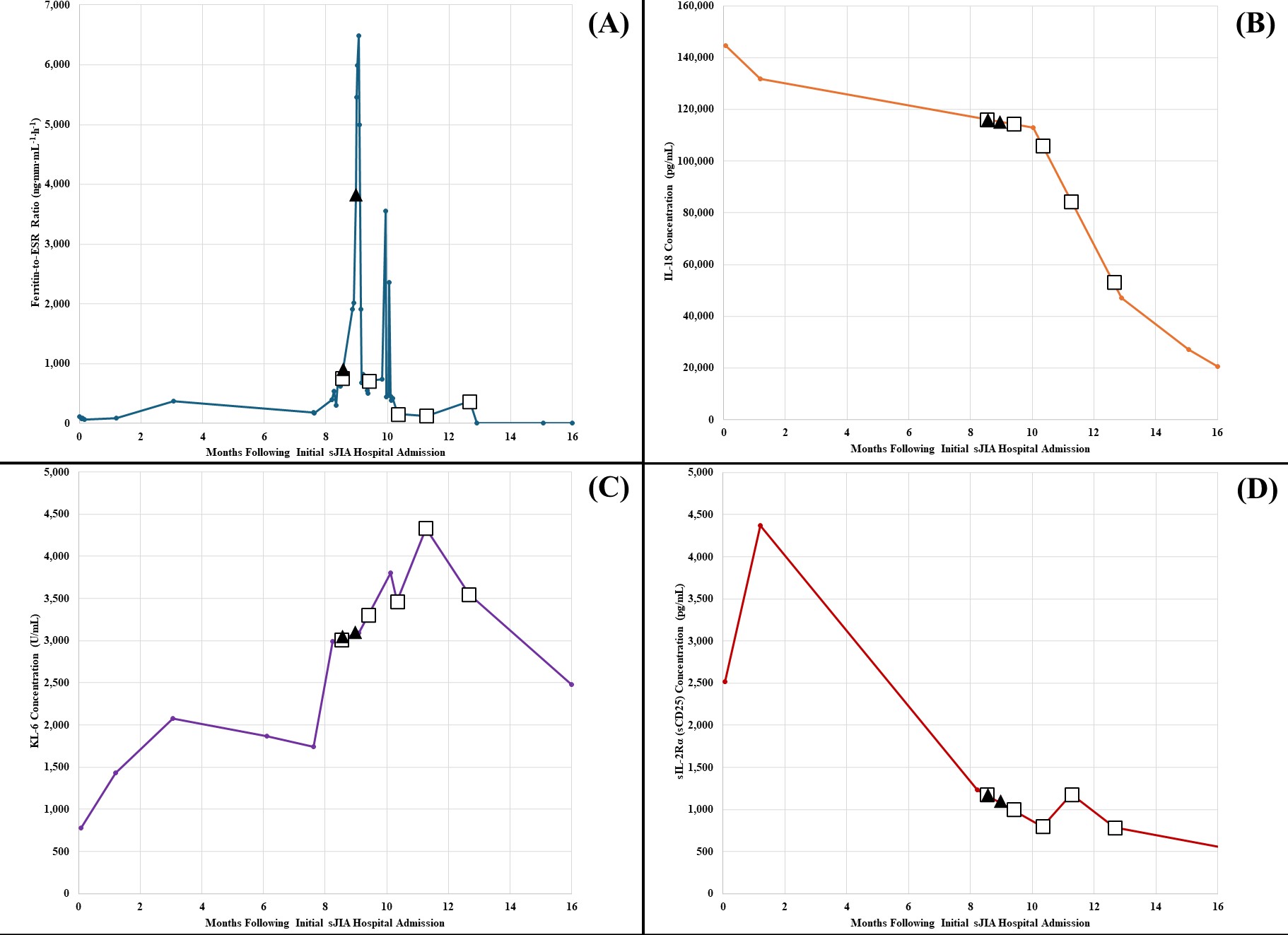 Black triangles represent dates of rituximab infusions. White squares represent dates of cyclophosphamide infusions. (A) Ferritin-to-ESR Ratio (ng∙mm∙mL-1∙h-1). (B) IL-18 Concentration (pg/mL). (C) KL-6 Concentration (U/mL). (D) sIL-2Rα (sCD25) Concentration (pg/mL). *ESR, erythrocyte sedimentation rate; IL-18, interleukin-18; KL-6, Krebs von den Lungen-6; sCD25, soluble cluster of differentiation 25; sIL-2Rα, soluble interleukin-2 receptor alpha (chain); sJIA-LD, systemic juvenile idiopathic arthritis-associated lung disease.
Black triangles represent dates of rituximab infusions. White squares represent dates of cyclophosphamide infusions. (A) Ferritin-to-ESR Ratio (ng∙mm∙mL-1∙h-1). (B) IL-18 Concentration (pg/mL). (C) KL-6 Concentration (U/mL). (D) sIL-2Rα (sCD25) Concentration (pg/mL). *ESR, erythrocyte sedimentation rate; IL-18, interleukin-18; KL-6, Krebs von den Lungen-6; sCD25, soluble cluster of differentiation 25; sIL-2Rα, soluble interleukin-2 receptor alpha (chain); sJIA-LD, systemic juvenile idiopathic arthritis-associated lung disease.
Case 2 sJIA-Associated Growth Failure and Recovery with Rituximab-Cyclophosphamide Therapy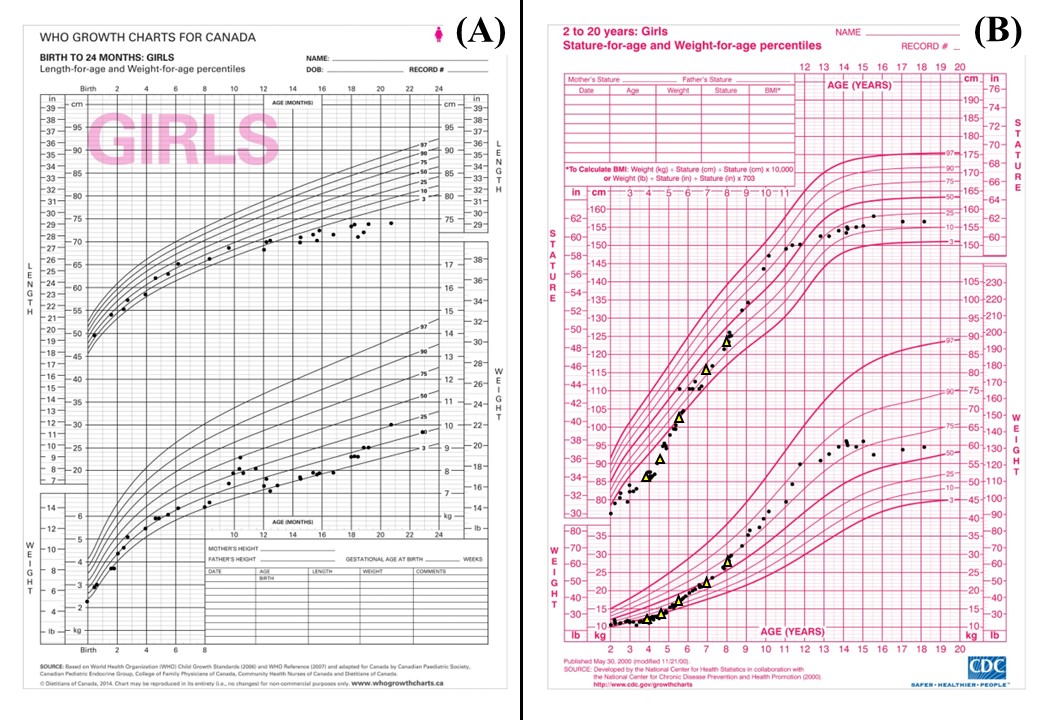 Yellow triangles represent dates of rituximab infusions. The patient received monthly cyclophosphamide infusions between the first and second rounds of rituximab infusions. Growth velocity significantly increased following induction on rituximab-cyclophosphamide combination therapy. (A) WHO 0-24 months. (B) CDC 2-20 years. *CDC, Centers for Disease Control; sJIA, systemic juvenile idiopathic arthritis; WHO, World Health Organization.
Yellow triangles represent dates of rituximab infusions. The patient received monthly cyclophosphamide infusions between the first and second rounds of rituximab infusions. Growth velocity significantly increased following induction on rituximab-cyclophosphamide combination therapy. (A) WHO 0-24 months. (B) CDC 2-20 years. *CDC, Centers for Disease Control; sJIA, systemic juvenile idiopathic arthritis; WHO, World Health Organization.
Case 1 Chest Computed Tomography Scan Prior to Rituximab-Cyclophosphamide Induction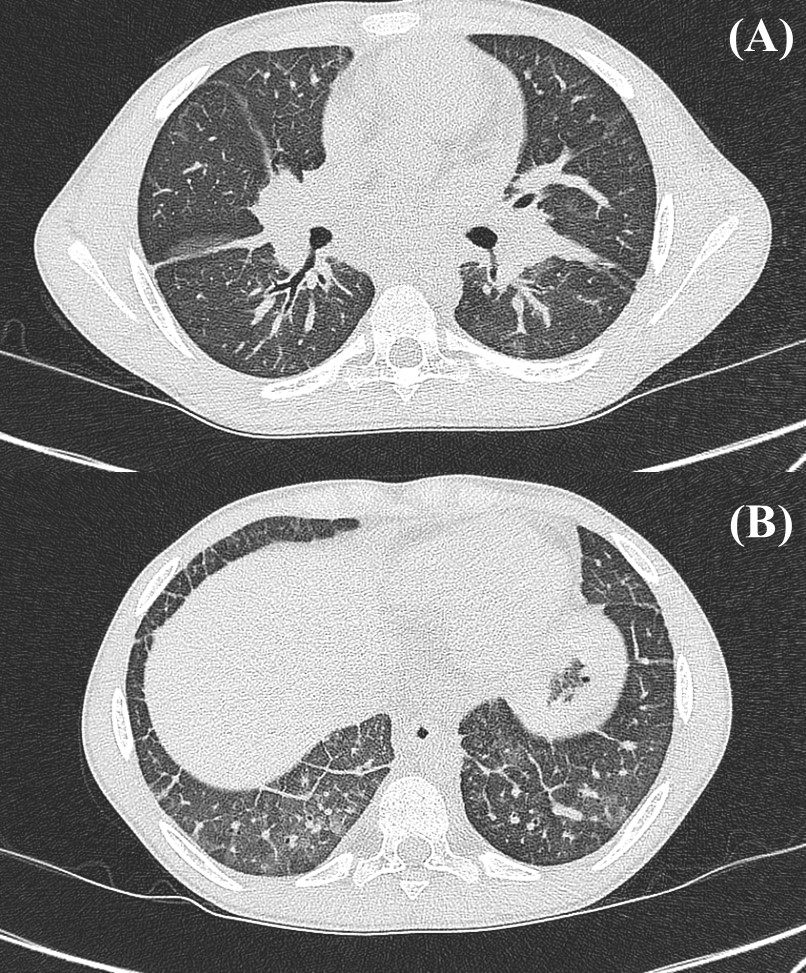 sJIA-LD characterized by the following: (A) Interlobular septal and peribronchial thickening. (B) Bronchiectasis and peribronchial thickening in the bilateral lower lobes. *sJIA-LD, systemic juvenile idiopathic arthritis-associated lung disease.
sJIA-LD characterized by the following: (A) Interlobular septal and peribronchial thickening. (B) Bronchiectasis and peribronchial thickening in the bilateral lower lobes. *sJIA-LD, systemic juvenile idiopathic arthritis-associated lung disease.
To cite this abstract in AMA style:
Freeman W, Cron R, Rife E. Case Series: Treatment of Refractory Lung Disease in Systemic Juvenile Idiopathic Arthritis with Cyclophosphamide and Rituximab Combination Therapy [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/case-series-treatment-of-refractory-lung-disease-in-systemic-juvenile-idiopathic-arthritis-with-cyclophosphamide-and-rituximab-combination-therapy/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/case-series-treatment-of-refractory-lung-disease-in-systemic-juvenile-idiopathic-arthritis-with-cyclophosphamide-and-rituximab-combination-therapy/