Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose:
Data regarding monogenic systemic autoinflammatory disorders (SAID) from the USA is scarce. Our study aims to report the spectrum of SAID and detail unique clinical phenotypes in patients living in Southeast Michigan.
Methods:
A single center retrospective study of medical records for patients diagnosed with genetically confirmed monogenic SAID over past five years.
Results:
Forty-nine patients (27 males, 23 females) were included into two categories: periodic fever syndromes and rare SAID. Familial Mediterranean Fever (FMF) was the most common periodic fever syndrome (n=39) with positive family history in 20/33 probands (94% of Middle Eastern descent). Thirty-five patients had classic FMF manifestations. Other manifestations included juvenile idiopathic arthritis (n=2), chronic nonbacterial osteomyelitis and sacroiliitis (n=2) overlapping PFAPA phenotype (n=1), Behcet disease (n=1), and one patient had coexisting cystic fibrosis. Most common MEFV mutations in 33 probands were p.M694V (n=17), p.V726A (n=11), p.M694I (n=4) and others (n=10) presenting as homozygous (n=6), heterozygous (n=23), and compound heterozygous (n=10) genotypes. Colchicine was used in n=30 and canakinumab in n=5. Other periodic fever syndromes included two other male siblings from one Hispanic kindred with TRAPS and one Caucasian female with NLRP12 related AID, all three patients are responsive to canakinumab. Rare SAID category included seven patients: 1) Yao syndrome in one female with recurrent fever and macrophage activation syndrome responsive to glucocorticoids and canakinumab, 2) two siblings from one Arabic kindred presenting with two distinct clinical monogenic lupus and vasculitis phenotypes (brother with class IV lupus nephritis, and sister with life threating pANCA related pulmonary hemorrhage) related to homozygous c.290_291del (p.Thr97Ilefs*2) pathogenic variant in DNASE1L3 gene, 3) one female from a three generation family with Blau syndrome with arthritis, rash and uveitis resistant to infliximab and canakinumab; partially responsive to adalimumab) , 4) one male with heterozygous PSTPIP1 p.Glu250Lys and MEFV p.V726A mutations diagnosed with PAPA and responsive to canakinumab, with family history of PAPA and renal failure in his father, and 5) one male and one female with Aicardi-Goutières syndrome presenting with SLE-like and systemic inflammatory disorders.
Conclusion:
Monogenic SAIDs often present with complex clinical phenotypes that can mimic other rheumatic entities and should be considered in patients with early age of onset of disease, severe clinical manifestations, rheumatic manifestations that are poorly responding to classic anti-rheumatic drugs, and variable rheumatic manifestations in multiple generations. Negative family history alone should not preclude doing genetic testing.
Spectrum of patients with Monogenic Autoinflammatory Disorders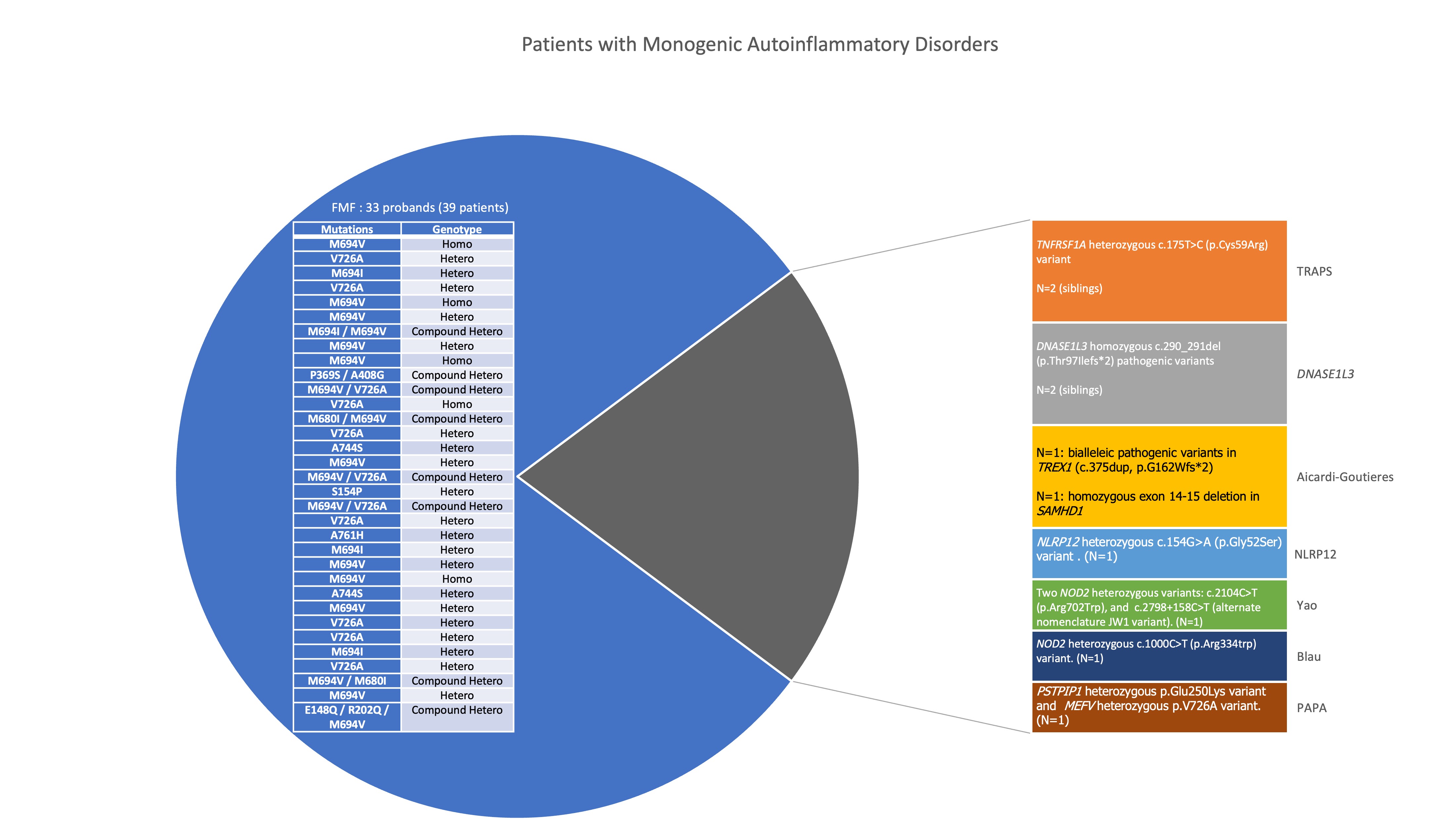 Homo: Homozygous, Hetero: heterozygous, Compound Hetero: Compound Heterozygous
Homo: Homozygous, Hetero: heterozygous, Compound Hetero: Compound Heterozygous
SLE and systemic inflammatory disorders associated with Aicardi-Goutières syndrome (AGS) 2A and 2B: A 10 months old male with AGS presenting with cutaneous manifestations on face and trunk leading to hypopigmentation . Patient serology at age 20 months was consistent with SLE including positive ANA and anti-smith antibodies.
2A and 2B: A 10 months old male with AGS presenting with cutaneous manifestations on face and trunk leading to hypopigmentation . Patient serology at age 20 months was consistent with SLE including positive ANA and anti-smith antibodies.
2C and 2D: A 10 years old female with AGS manifesting with severe vasculopathy of extremities and livedo reticularis with elevated ESR but negative SLE serology.
Three generation family with Blau Syndrome 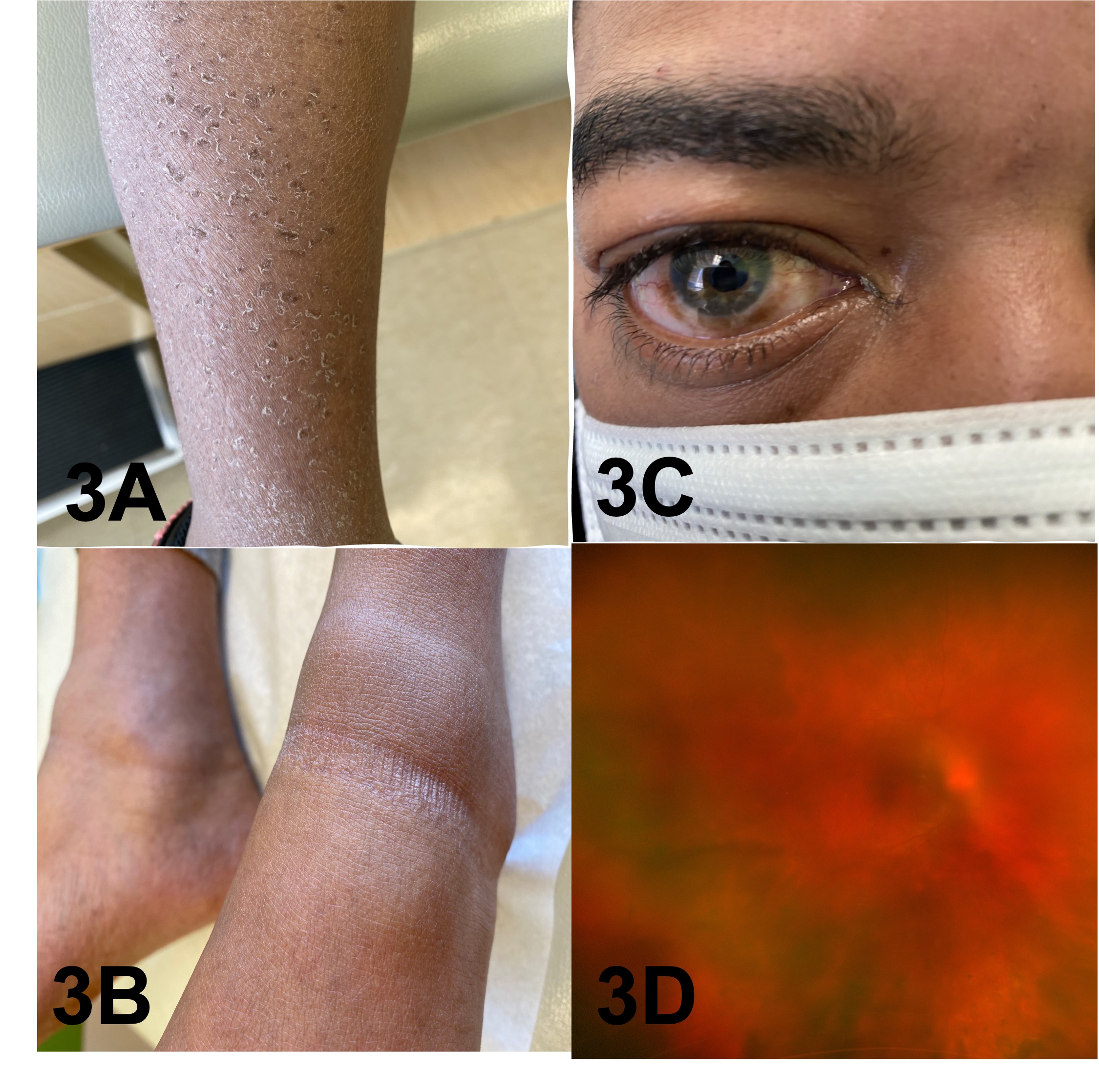 3A and 3B: A 7-year-old female with polyarthritis initially diagnosed with seronegative polyarticular juvenile idiopathic arthritis (JIA) resistant to treatment. She eventually developed ocular or cutaneous manifestations.
3A and 3B: A 7-year-old female with polyarthritis initially diagnosed with seronegative polyarticular juvenile idiopathic arthritis (JIA) resistant to treatment. She eventually developed ocular or cutaneous manifestations.
3C and 3D: The father of the patient with severe bilateral panuveitis and glaucoma.
To cite this abstract in AMA style:
Mitacek R, Kwiatkowski V, Fathalla B. Genotypes and Clinical Phenotypes of Monogenic Autoinflammatory Disorders in Michigan [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/genotypes-and-clinical-phenotypes-of-monogenic-autoinflammatory-disorders-in-michigan/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/genotypes-and-clinical-phenotypes-of-monogenic-autoinflammatory-disorders-in-michigan/