Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose: Kawasaki disease (KD) is an acute medium-vessel vasculitis predominantly affecting children younger than five years old. It is the most common cause of acquired heart disease in developed countries due to risk of developing coronary artery aneurysms (CAAs). Giant CAAs occur in only 0.2–2% of KD patients but represent a major cause of morbidity. While outcomes have improved since the standardization of early IVIg therapy, optimal treatment for giant CAAs remains unclear. We describe the presentation, treatment, and outcomes of patients with KD-associated giant CAAs at our large center with a diverse population.
Methods: With IRB approval, we conducted a retrospective study of children diagnosed with KD with giant CAAs from 1/1/17-12/31/24. Demographics, clinical features, laboratory and imaging findings, and treatments were recorded. Data were reported as frequencies and proportions for categorical variables and as median and interquartile range (IQR) for continuous variables.
Results:
During the defined period, out of approximately 900 patients admitted with KD, 29 developed giant CAAs. Patients with giant CAAs were diagnosed and treated with IVIg on median day nine of fever (IQR 6-14). Median age of diagnosis was 1.2 years (IQR 0.5-3), sex distribution was equal, and most patients were of Hispanic ethnicity (Table 1).
Fifteen patients (52%) met complete KD criteria, and 14 patients (48%) met incomplete KD criteria. Five (17%) presented with KD shock syndrome. Patients had a median of four echocardiograms (IQR 3-12) during admission. Twenty-four patients (83%) underwent CTA or MRA while admitted for additional CAA characterization.
Giant CAAs were noted in five (17%) in the left main coronary artery (LCA), 14 (48%) in the right coronary artery (RCA), and 18 (62%) in the left anterior descending artery (LAD). Seven (24%) had two giant CAAs and one (3%) had three.
Steroids were the first choice for primary intensification; 13 (45%) received steroid within 24 hours of IVIg. All were treated with IVIg and steroid, and 21 (70%) were treated with pulse steroid (30 mg/kg). Three were treated with IVIg and steroid only. Additional immune modulatory use varied widely (Figure 1).
Regarding anticoagulation, all patients were treated with aspirin, 16 (55%) with low molecular weight heparin, 14 (48%) with clopidogrel, one (3%) with heparin, and one (3%) with TPA.
Major acute cardiac complications include one episode of arrhythmia and one arrest. Late complications included one patient with suspected RCA thrombus, one with RCA occlusion for which reperfusion was not attempted, and one with RCA thrombus requiring tPA. Over a median follow up period of 2.4 years (IQR 1.5-6.3), 13 (44%) had resolution of giant aneurysm defined by z-score normalization.
Conclusion:
In this single center cohort of patients with KD-associated giant CAAs, immune modulatory treatments varied widely, and rates of regression were higher than previously reported. Although nearly half of aneurysms regressed over time, significant cardiac and thrombotic complications still occurred.These findings highlight the need for future studies to define optimal therapy and validate predictive markers for CAA development to improve outcomes for children with KD.
Table 1. Patient characteristics.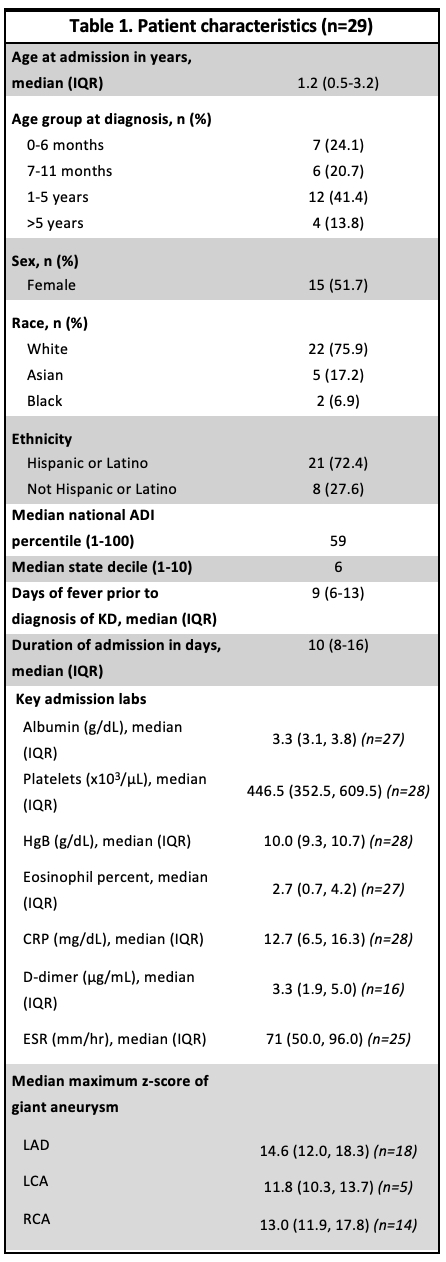
Figure 1. Summary of additional therapies.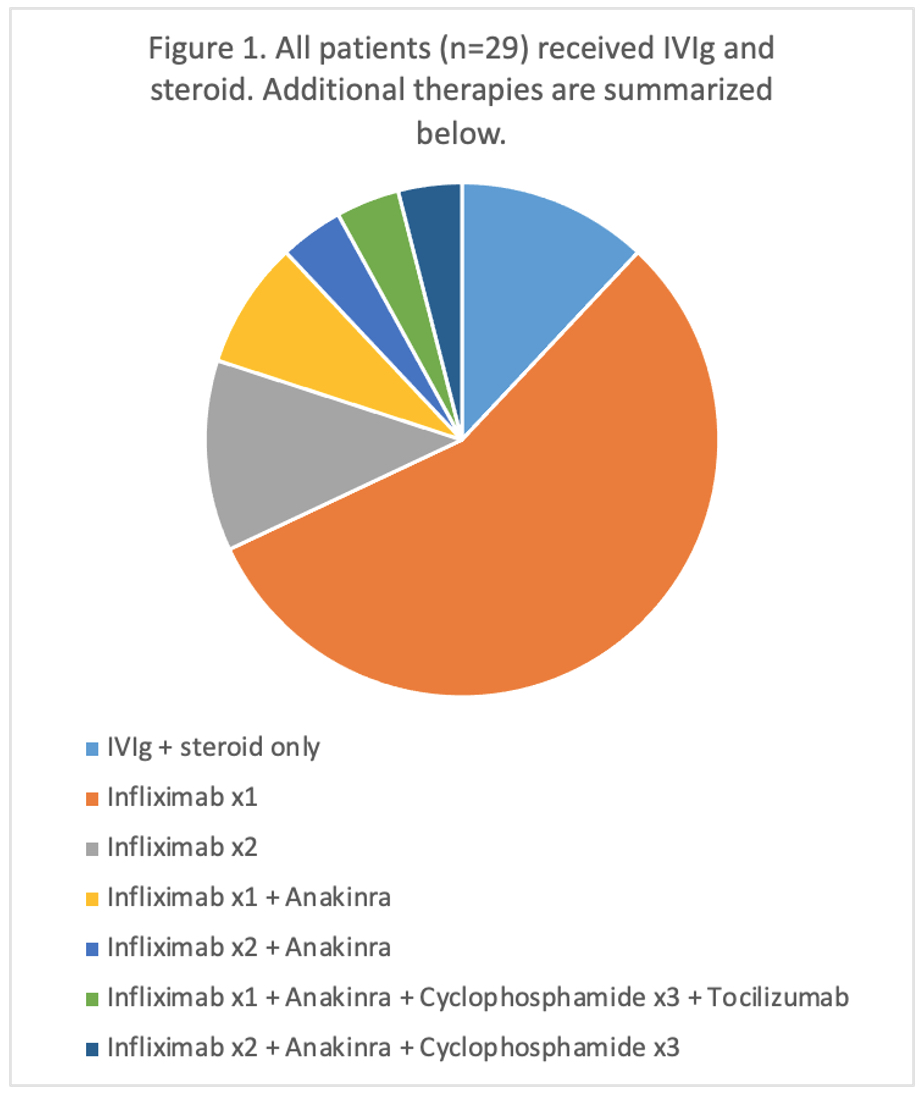
Figure 2. Proportion of normalization of z-score of giant aneurysm grouped by additional immune modulatory treatments. 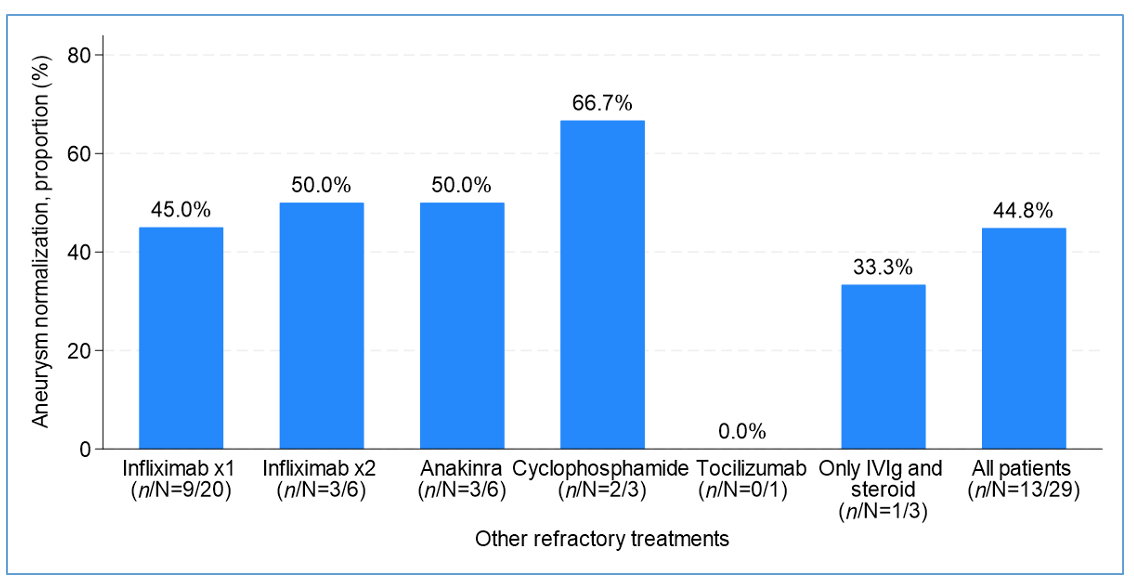
To cite this abstract in AMA style:
Rae M, Nguyen J, Kwan O, Nguyen D, Yildirim-Toruner C. Giant Aneurysms in Kawasaki Disease: A Large Quarternary Single Center Experience [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/giant-aneurysms-in-kawasaki-disease-a-large-quarternary-single-center-experience/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/giant-aneurysms-in-kawasaki-disease-a-large-quarternary-single-center-experience/