Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose: Systemic juvenile idiopathic arthritis (SJIA) shows heterogeneous disease trajectories, and the subset of patients who achieve remission with methotrexate (MTX) monotherapy is not well defined. MTX remains widely used in resource-limited settings, yet most published data suggest limited durability as monotherapy. This study aimed to characterize clinical, laboratory, and longitudinal features associated with MTX-only versus MTX-plus treatment courses in a large tertiary-care cohort.
Methods: A retrospective analysis was conducted (July 2001 – September 2025) on patients diagnosed with SJIA (ILAR 2001 criteria) before age 18 with ≥2 years of follow-up. Clinical features and laboratory investigations, at presentation, and disease variables (age at onset, time to diagnosis, time to remission, flares, MAS events) were extracted from clinical records. Outcomes included remission on drugs, remission off drugs, active disease, and disease course patterns (monocyclic, polycyclic, persistent). Corticosteroid exposure (oral, IV), intra-articular steroids, and all DMARD use were recorded. All patients received MTX and were stratified as MTX-only or MTX-plus (additional DMARDs/biologics), and compared.
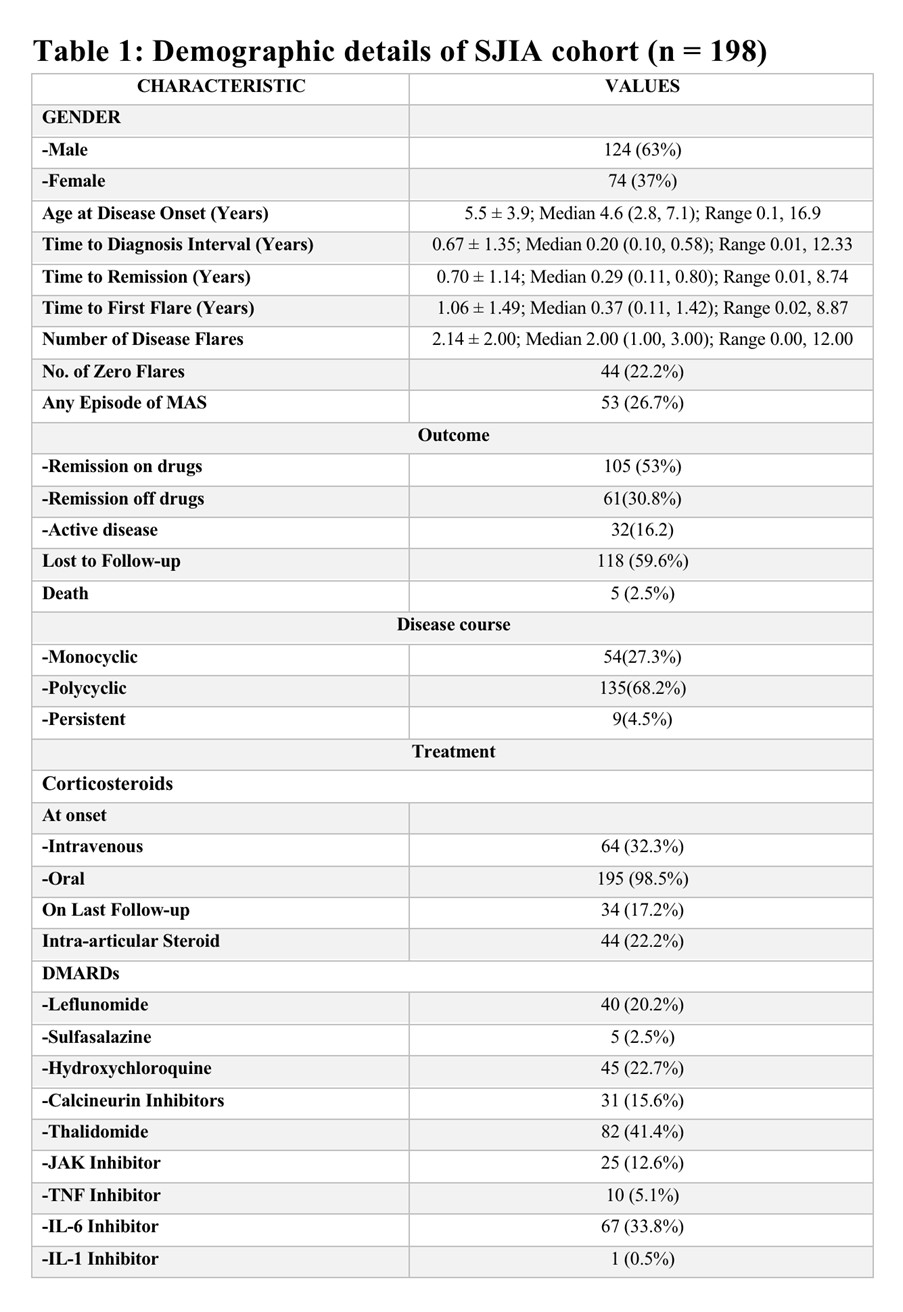
Results: Among 198 patients (mean onset age 5.8 ± 3.8 yrs; median follow-up 5.5 [3.5, 8.7] yrs; 63% male), key onset features were fever (100%), arthritis (98%), rash (69%), lymphadenopathy (35%), hepatomegaly (20%), splenomegaly (14%), and serositis (4%), with MAS in 26.7%; with 5 deaths. All received steroids (32.3% IV, 98.4% oral), and at last follow-up remission off/on drugs and active disease were 30.8%, 53%, and 16.2%, respectively (see Table 1).
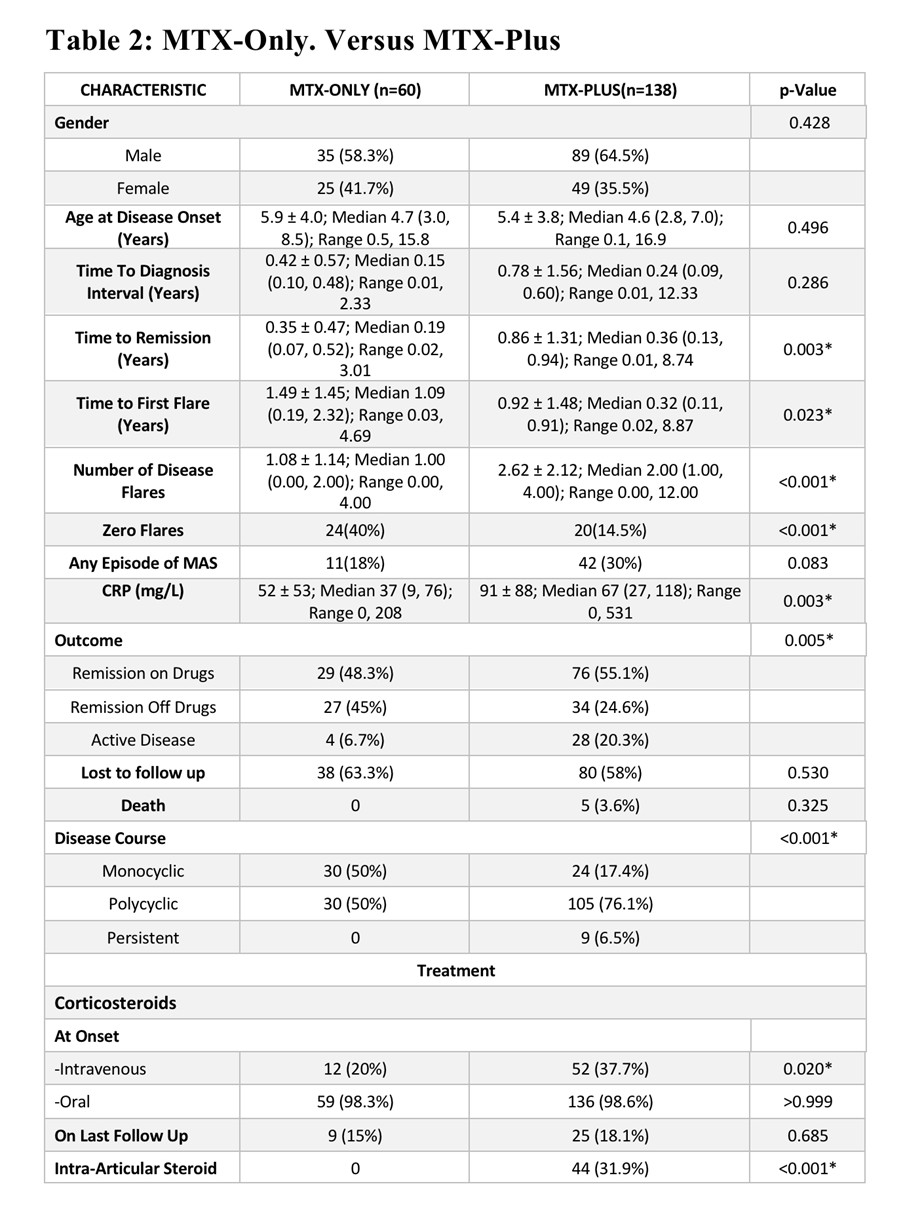
MTX-only (n=60) and MTX-plus (n=138) groups differed, with MTX-plus showing longer follow-up (7.2 vs 4.8 yrs), time to remission (0.86 vs 0.35 yrs), earlier first flare (0.32 vs 1.09 yrs), and longer MTX duration (6.4 vs 3.9 yrs), but similar peak dose (0.75 vs 0.72 mg/kg/week); remission patterns, disease courses, and flare frequency differed significantly, with zero-flare disease more frequent in MTX-only (40% vs 14.5%) (see Table 2).
Conclusion: In this tertiary-care cohort, about 1/3rd of patients sustained remission with MTX monotherapy, demonstrating a distinct MTX-responsive phenotype, despite prevailing literature favoring early biologic escalation. MTX-only patients had faster remission, fewer flares, more monocyclic disease, and better long-term drug-free remission rates compared with MTX-plus patients, who experienced more flares and prolonged disease activity despite similar MTX dosing. These findings highlight clinically recognizable divergence in SJIA disease trajectories and support data-driven stratification of MTX use in real-world settings.
To cite this abstract in AMA style:
Mittal M, Rajpal N, Agarwal m, Sawhney s. Methotrexate Response in Systemic JIA: Real-World Evidence from a Tertiary-Care Cohort [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/methotrexate-response-in-systemic-jia-real-world-evidence-from-a-tertiary-care-cohort/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/methotrexate-response-in-systemic-jia-real-world-evidence-from-a-tertiary-care-cohort/