Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose: Kawasaki disease (KD) is a systemic medium vessel vasculitis that is predominantly a clinical diagnosis as defined by the American Heart Association (AHA). KD is the most common cause of acquired heart disease in children with 25% of untreated cases developing coronary artery aneurysms (CAAs). Majority of cases occur in children < 5 years of age. In younger infants, the immune system is immature and classic symptoms of KD are often absent leading to a misdiagnosis or delay in diagnosis. This is the age group where chances of CAA are highest. Complications of CAA include stenosis formation, coronary thrombosis, myocardial infarction, and sudden death. Giant aneurysms have fatal risk of rupture. In this study, we identified infants with KD 6 months or younger and compared them to those over 6 months.
Methods: Retrospective multicentric observational study of infants ≤12 months diagnosed with KD. Patients included from 2 centres: Neoclinic Children’s Hospital, Jaipur and Sir Ganga Ram Hospital, New Delhi between April 2019 to June 2025. Diagnosis was based on AHA 2017 or clinical for incomplete KD. 2D ECHO done by different Paediatric cardiologists on different ECHO machines; CAA z scores calculated using either Dallaire and Dahdah or Boston formula. Data collected included demographics, clinical features, echocardiography findings & treatment outcomes. Continuous variables summarized using medians and ranges; categorical variables summarized as counts and percentages. Categorical variables analysed using Fisher’s Exact Test. Continuous variables compared using Mann-Whitney U test. Statistical significance defined as p < 0.05. Analysis performed using standard SPSS statistical software.
Results: Younger Infants< 6 mnths (Group A) had significantly higher rates of abnormal CAA (94.4%) compared to older infants (Group B) (61.1%), with significant differences in CAA favouring Group B (p ≈ 0.04). Incomplete KD present in all infants of Group A (100%) and 12/18 (66.7%) in Group B. Median age at onset 3 months in Group A vs. 10 months in Group B. Median delay in diagnosis similar (11.5 vs 12.5 days). Fever & irritability universal in both groups. Certain features, such as red dry lips, were more common in Group B (12/18) than Group A (5/18) with p = 0.044. Other clinical symptoms showed no significant differences. Male predominance was higher in Group B compared to Group A. Rates of primary intensification and steroid-resistant disease after intensification were similar in both groups. The proportion of infants managed with only IVIG and moderate dose aspirin who were resistant was comparable ( Table 1).Median delay in diagnosis more with worse CAA & those infants required primary intensification(Table 2).
Conclusion: Almost all infants presented with incomplete disease (fever and irritability predominant) often leading to delay in diagnosis & high risk for CAA & long term cardiac sequale. The distribution showed a greater proportion of normal coronaries in older infants; infants < 6months had more CAA with Z score >2.5 indicative of higher disease burden. Pediatricians need to identify infants requiring earlier and more aggressive intervention. Larger studies with Indian infants are required to confirm these findings.
Clinical profile of infants with KD younger than 6 months (group A) compared to 7-12months (Group B)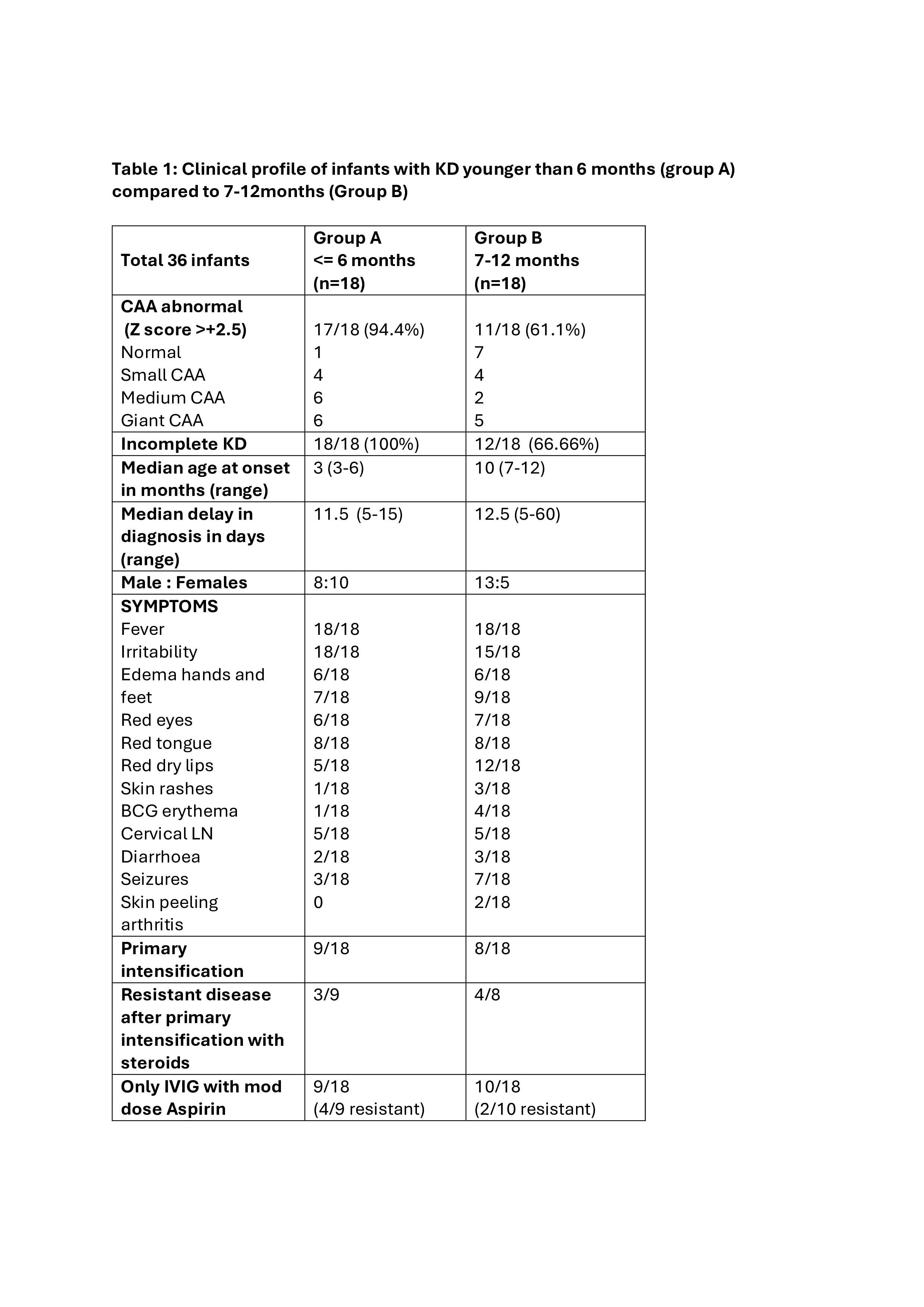
Comparison of infants with normal-small aneurysms with medium-large aneurysms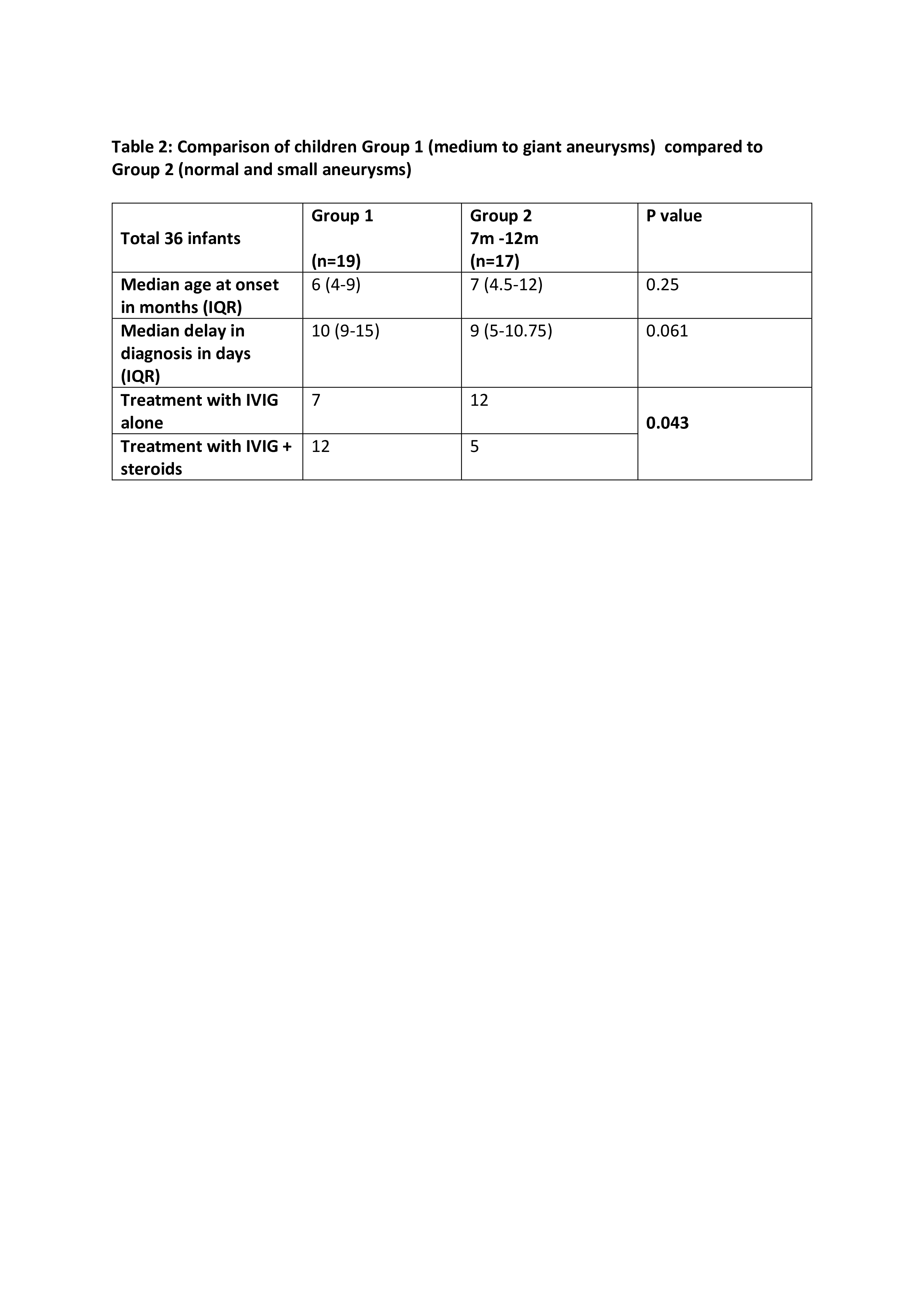
To cite this abstract in AMA style:
Shivpuri A, Agarwal m, Sawhney s. Age Matters: Clinical Profile and IVIG Responsiveness in infants with Kawasaki Disease. A multicentric retrospective analysis of 36 patients from North India [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/age-matters-clinical-profile-and-ivig-responsiveness-in-infants-with-kawasaki-disease-a-multicentric-retrospective-analysis-of-36-patients-from-north-india/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/age-matters-clinical-profile-and-ivig-responsiveness-in-infants-with-kawasaki-disease-a-multicentric-retrospective-analysis-of-36-patients-from-north-india/