Session Information
Date: Thursday, March 19, 2026
Title: Plenary Abstract Session I
Session Time: 2:30PM-2:45PM
Background/Purpose: The cumulative impact of childhood-onset systemic lupus erythematosus (cSLE) on cardiovascular damage begins at disease onset. We sought to characterize longitudinal cardiovascular profiles of youth with cSLE. Herein we report patterns of ambulatory blood pressure (BP) and other cardiovascular disease (CVD) risk factors over time.
Methods: Participants 9-21 years of age, meeting ACR or ACR/EULAR classification criteria for SLE with disease onset before age 18, were prospectively enrolled from two centers (2020-2025) to undergo serial cardiovascular testing. Peripheral arterial tonometry and 24-hour oscillometric ambulatory BP monitoring (ABPM) were performed at baseline, 6 and 18 months, while transthoracic echocardiograms, carotid ultrasounds, and fasting biosamples were obtained at baseline and 18 months. Ambulatory hypertension (elevated clinic and ambulatory BP), masked hypertension (normal clinic BP with elevated ambulatory BP), non-dipping BP (< 10% decrease in BP during sleep), and reverse dipping (higher BP in sleep vs. wake periods) were categorized by the 2022 American Heart Association classification. We used mixed effects models adjusted for disease activity (SLEDAI-2K) and oral glucocorticoid dose to evaluate changes in ambulatory BP over time.
Results: We enrolled 37 participants with median age of 17.0 [IQR 14.7–16.7], disease duration of 1.5 years [0.4–4.4], and SLEDAI-2K of 4 [2.0–6.0] (Table 1). 10 (27%) had nephritis and 9 (24%) were on anti-hypertensive medications at baseline. 11 (29%) did not complete all study visits (withdrew, lost to follow-up). Among 76 evaluable ABPM tracings, hypertension classification by ambulatory vs. clinic BP was discordant 25% of the time (Table 2). Prevalence of masked hypertension was 25% (8/32), 22% (6/27) and 24% (4/17) at baseline, 6 and 18 months, respectively, including 4 patients that developed masked hypertension during follow-up. The overall prevalence of hypertension was 34% at baseline, with no significant decrease in odds of hypertension at 6 or 18 months vs. baseline. At baseline, 21 (66%) and 8/32 (25%) participants had non-dipping SBP and DBP, respectively; 3 had reverse dipping. SBP non-dipping tended to improve during follow-up, though 3 participants transitioned from normal SBP dipping to non-dipping (Fig. 1A). Similar patterns were observed with DBP dipping, though DBP non-dipping was less common overall (Fig. 1B). There was a significantly decreased likelihood of non-dipping at 18 months vs. baseline (OR 0.07, 95% CI 0.01-0.65), adjusted for disease activity and glucocorticoid dose. Dyslipidemia was present in 44% of participants at baseline. Low HDL was most common (53%), followed by hypertriglyceridemia (47%) and elevated LDL (19%). There was no change in prevalence of dyslipidemia from baseline to 18 months (44%).
Conclusion: In youth with cSLE, CVD risk is dynamic and multifactorial. Masked hypertension and dyslipidemia are highly prevalent CVD risk factors that frequently persist and are insufficiently controlled. Monitoring ambulatory BP and other modifiable CVD risk factors longitudinally in this population can facilitate early intervention to prevent accrual of target organ damage.
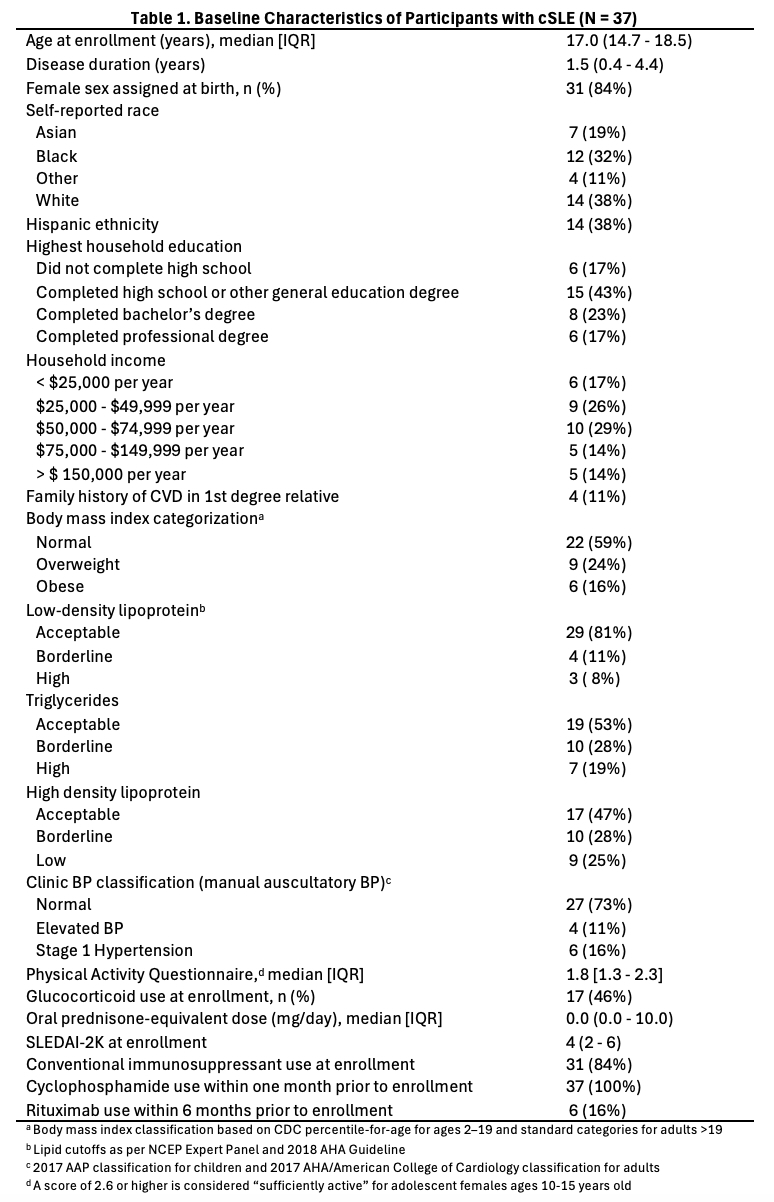
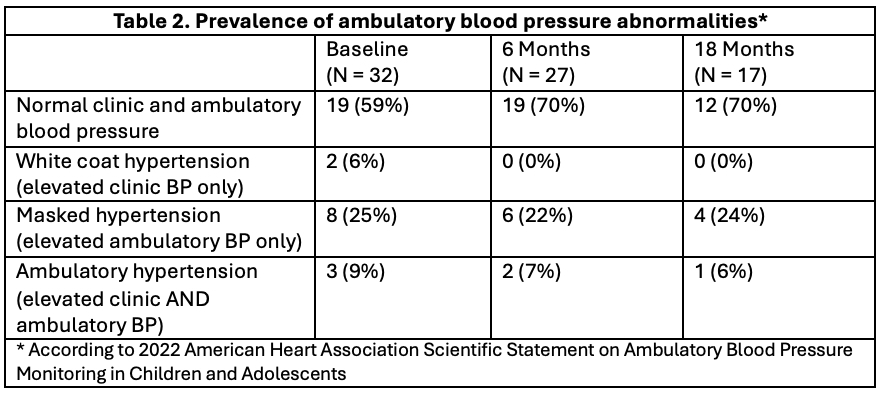
Figure 1. Longitudinal changes in nocturnal blood pressure dipping patterns in youth with cSLE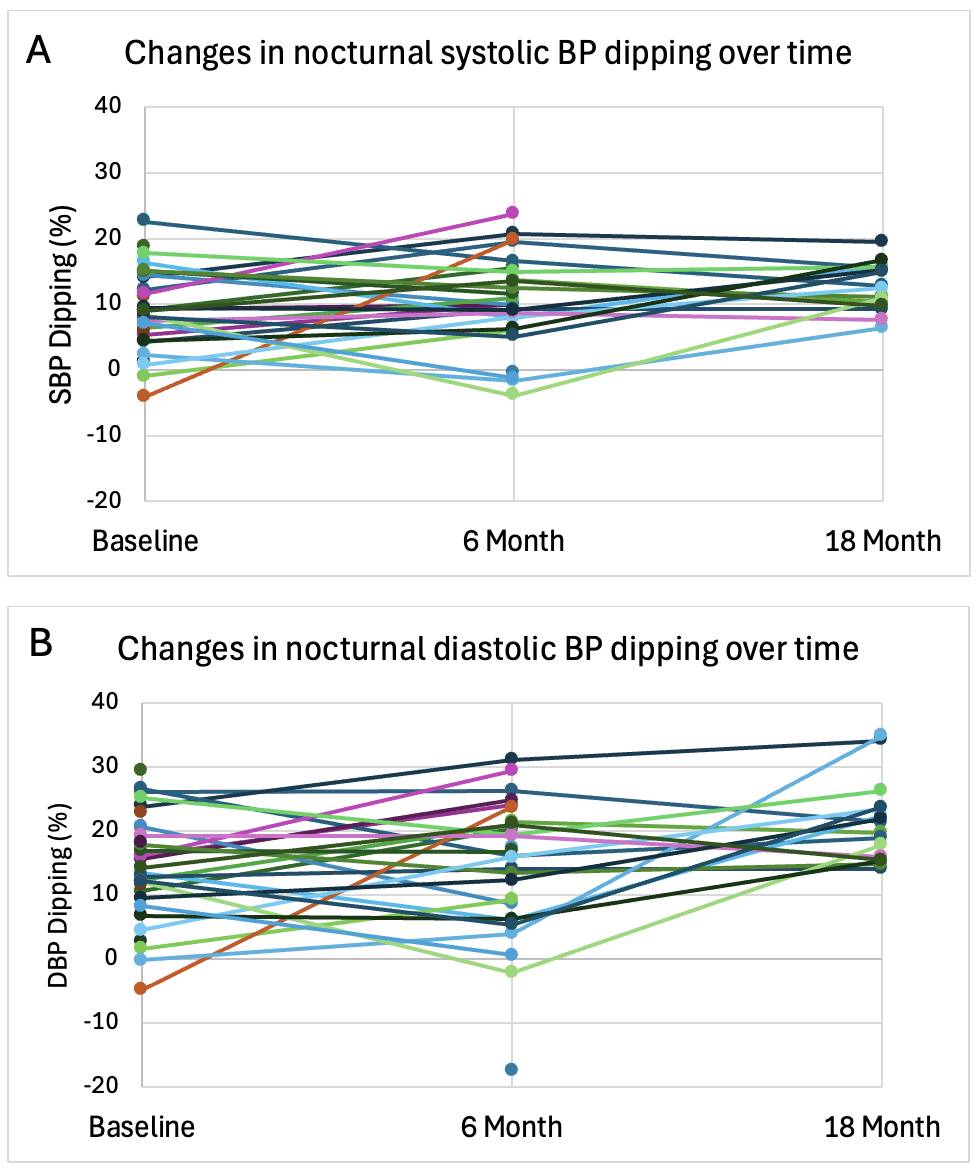 Figure 1 Legend. Longitudinal patterns of diurnal blood pressure (BP) variation as represented by the percentage decrease from daytime to nighttime in A) systolic and B) diastolic BP measurements obtained via 24-hour ambulatory blood pressure monitoring. Each line represents an individual participant. Only measurements from evaluable ABPM tracings are represented (device worn for the full 24 hours without documentation of significant sleep disruption). Normal dipping is defined by a decrease of >10% from daytime to nighttime. Negative values represent reverse dipping (higher BP at night vs. daytime).
Figure 1 Legend. Longitudinal patterns of diurnal blood pressure (BP) variation as represented by the percentage decrease from daytime to nighttime in A) systolic and B) diastolic BP measurements obtained via 24-hour ambulatory blood pressure monitoring. Each line represents an individual participant. Only measurements from evaluable ABPM tracings are represented (device worn for the full 24 hours without documentation of significant sleep disruption). Normal dipping is defined by a decrease of >10% from daytime to nighttime. Negative values represent reverse dipping (higher BP at night vs. daytime).
To cite this abstract in AMA style:
Chang J, Alonzi G, Ferguson M, Knight A, Newburger J, Weiss P, Son M, Costenbader K. Longitudinal Cardiovascular Profiles of Youth with Childhood-onset Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/longitudinal-cardiovascular-profiles-of-youth-with-childhood-onset-systemic-lupus-erythematosus/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/longitudinal-cardiovascular-profiles-of-youth-with-childhood-onset-systemic-lupus-erythematosus/