Session Information
Date: Monday, October 27, 2025
Title: (1612–1632) Vasculitis – Non-ANCA-Associated & Related Disorders Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Advances in imaging modalities has led to increased diagnosis of aortitis. While aortitis occurring in the setting of giant cell arteritis (GCA) and Takayasu arteritis (TAK) is well characterized, other forms of aortitis are less well characterized and can be associated with a variety of other etiologies or may be idiopathic. We sought to identify the demographic, clinical and imaging characteristics of non-GCA/TAK aortitis.
Methods: In this retrospective cross-sectional study, the study population was identified using ICD 10 codes for aortitis from 1/1/12-12/31/22, across NYU Health system. Eligibility criteria were age between 18-90 years and a diagnosis of aortitis. 300 subjects were identified by using EMR diagnoses of aortitis, GCA, TAK. All charts were reviewed by rheumatology and radiology teams. 52 cases met the inclusion criteria. For data analysis used Wilcoxon rank sum test for continuous variables and Fisher’s exact test for categorical variables. A p-value of < 0.05 was considered statistically significant. All analyses were performed using R (R Core Team) version 4.4.0.
Results: 36 cases of non-GCA/TAK aortitis and 16 cases of TAK/GCA aortitis were identified. Of the TAK/GCA group, 44% were identified as GCA and 56% were identified as TAK. Of the non-GCA/TAK aortitis cases, 25% were associated with other autoimmune diseases such as ANCA-related disease, Bechet’s, RA, Sarcoid and SPA. In addition, 39% of the non-GCA/TAK cases were associated with infection and 36% were idiopathic. The median age for the non-GCA/TAK and GCA/TAK groups was 69 years and 45 years, respectively (p=0.002). 45% of aortitis cases were incidental findings. When patients did present with symptoms, 42% of non-GCA/TAK patients presented with abdominal pain and 33% with back pain (p=0.05). CTA/ CT was the most frequently utilized imaging modality in both groups. MRA/ MRI was utilized in 48% of cases for follow up purposes. Common imaging findings associated with aortitis included periaortic fat stranding and inflammatory changes which were seen in more than 54% of GCA/TAK aortitis and 52% of non-GCA/TAK aortitis cases (p=NS). Aortic wall thickening, which was seen in 77% of GCA/TAK aortitis cases and 64% of non-GCA/TAK aortitis p=NS. Aortic wall enhancement was seen in 54% of GCA/TAK aortitis cases vs 37% of non-GCA/TAK cases p=NS. Aortic stenosis was seen in 25% in GCA/TAK patients vs 2.8% non-GCA/TAK patients p=0.03. 70% of study participants received medical treatment for aortitis (85% of GCA/TAK cases and 69% of non-GCA/TAK cases). Steroids were used to treat over 66% of study participants; 87% in the GCA/TAK group and 55% in the non-GCA/TAK group (p=0.054).
Conclusion: In our health system cohort of aortitis cases, 45% were incidental findings. In non-GCA/TAK aortitis, 39% were attributed to infection, 25% to autoimmune conditions and 36% were idiopathic. Steroids, when employed for treatment of aortitis, were more commonly used in GCA/TAK aortitis vs non-GCA/ TAK aortitis. The difference may reflect caution regarding steroids use in cases of infectious aortitis as well some uncertainty regarding approach to treatment for non-GCA/TAK aortitis.
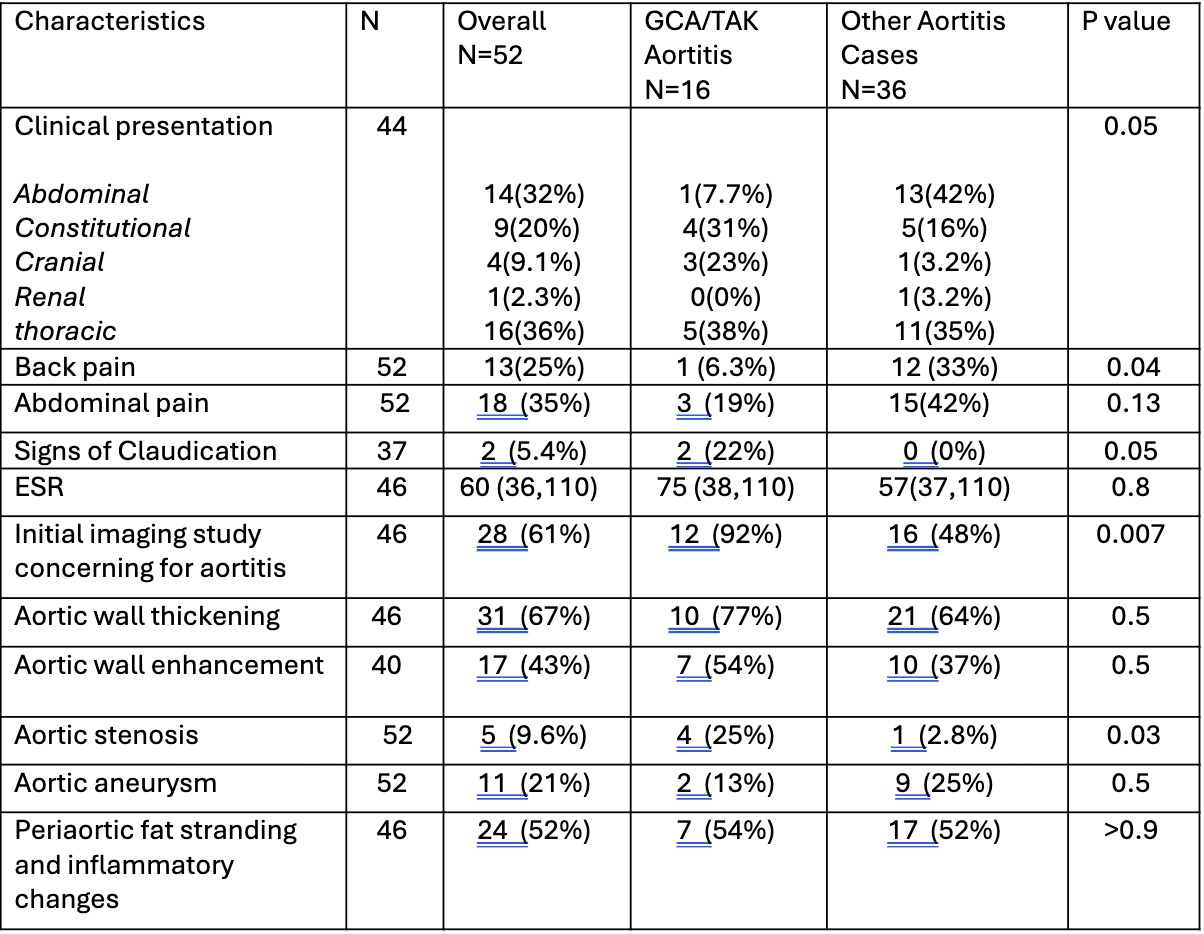 Table 1
Table 1
.jpg) Table 2
Table 2
.jpg) Table 3
Table 3
To cite this abstract in AMA style:
Batool N, Anwar Z, Hasan S, Tembelis M, Hoffmann J, Gencerliler N, Joseph j, Carsons S, Belilos E. Characterization of non-GCA, non-Takayasu Aortitis in a Single Health System Cohort [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/characterization-of-non-gca-non-takayasu-aortitis-in-a-single-health-system-cohort/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/characterization-of-non-gca-non-takayasu-aortitis-in-a-single-health-system-cohort/