Session Information
Date: Monday, October 27, 2025
Title: (1221–1247) Pain in Rheumatic Disease Including Fibromyalgia Poster
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Fibromyalgia (FM) and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) are prototypical nociplastic disorders marked by centralized pain & fatigue, respectively. Nociplastic symptoms — such as fatigue, psychological distress & dysautonomia — commonly complicate rheumatologic diseases and remain difficult to treat, thus highlighting the need for safe, effective & affordable therapies. Vestibulocortical stimulation (VCS) via caloric irrigation is a non-invasive neuromodulation technique that has demonstrated rapid analgesic effects in treatment-resistant nociplastic pain (Figure 1).1 This study aimed to replicate recent findings of VCS-induced analgesia in FM2 and assess its broader impact on quality of life to inform the design of randomized placebo-controlled trials.
Methods: We conducted a non-randomized open-label effectiveness trial in 39 patients with nociplastic pain & fatigue (mean age = 40.2; 87% female). Twenty-three patients met criteria for ME/CFS (2015 IOM criteria) and 16 met criteria for FM (2011 ACR criteria) +/- ME/CFS. Each participant completed validated electronic patient-reported outcomes at baseline, prior to receiving a single treatment of unilateral right-ear cold-water (4°C) irrigation at 1-2 cc/second. Pain & quality of life measures were reassessed at post-intervention 30 minutes, 1 day, 1 week, 2 weeks & 4 weeks.
Results: Regarding pain, 27 of 39 participants reported significant baseline pain intensity (≥4/10). At 30 minutes post-VCS, it significantly decreased (t(26) = -3.46, p = 0.002; Figure 2A) with 30% reporting ≥30% relief and 22% reporting ≥50% relief. At 24 hours post-VCS, 41% achieved ≥30% pain reduction and 37% reported ≥50% improvement (Figure 2B), with significant reductions also found in pain intensity (t(35) = -4.36, p < 0.001) and pain interference (t(35) = -3.67, p < 0.001; Figure 2C). Beyond 24 hours, no significant changes were observed as the study was underpowered to detect effects beyond that timeframe.Subjective well-being scores increased significantly post-VCS (t(37) = 3.89, p < 0.001; Figure 3A) and autonomic symptom burden (COMPASS-31) decreased over time (F(3,60) = 7.998, p < 0.001; Figure 3B). PROMIS-29 domains showed sustained improvements in anxiety & social role participation at 1, 2, and 4 weeks post-intervention. Fatigue levels remained unchanged and no major adverse events occurred. VCS was safe & well tolerated, with 86.1% of participants reporting a willingness to have the procedure repeated if it reduced pain by half for one week.
Conclusion: These findings provide further open-label trial evidence that VCS offers meaningful relief in nociplastic pain. This study is also the first to show proof-of-concept improvements in autonomic symptoms & quality of life following VCS in nociplastic disease. Large randomized placebo-controlled trials are needed to validate & further advance this simple, bedside procedure into therapeutic standard of care for millions of patients globally suffering with refractory rheumatologic & nociplastic disease.REFERENCESNgô T & Kaplan M. Australian Association of Musculoskeletal Medicine (AAMM) conference, 2023.Kaplan M et. al. Pain Med, 2024.
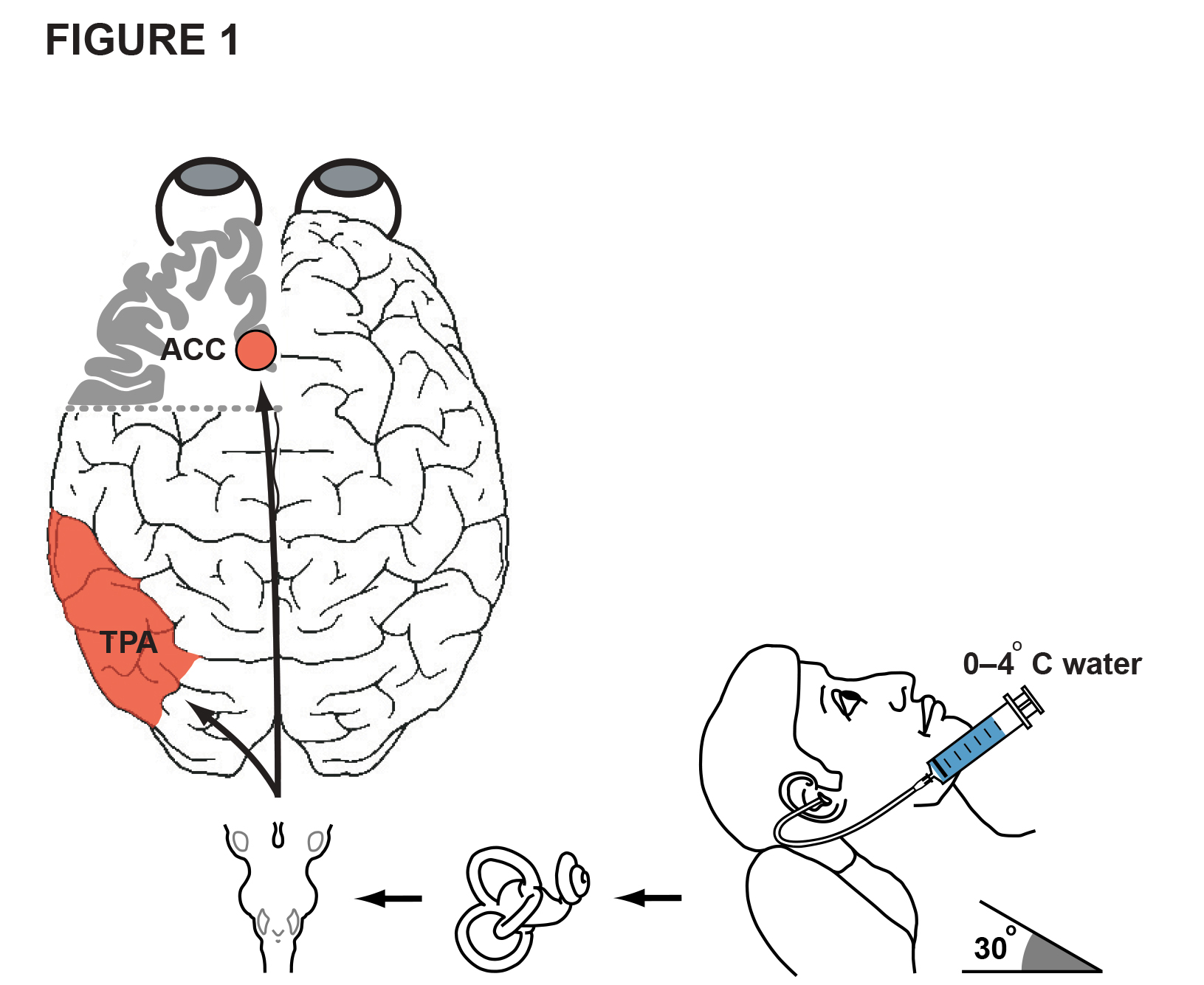 Figure 1: VCS with Caloric Irrigation — From Neurodiagnostic Technique to Therapeutic Neuromodulation Modality. The caloric test — via the vestibulo-ocular reflex — is a simple, low-cost, low-risk, non-invasive and widely used mainstream neurodiagnostic technique for balance problems & brain death, with a long-standing record of safety since its development over a century ago. The technique is routinely performed for example in primary care clinics by family doctors & nurses (for cerumen removal), audiologists, neurologists & ENT physicians. VCS involves irrigation of the external ear canal with warm/cold water (e.g., 1–4° C) while the head is reclined at 30° to the horizontal until nystagmus is observed and vertigo is reported — typically within a few seconds — via stimulation of semicircular canals & brainstem circuits (indicated by the black horizontal arrows). Over recent decades, several brain-imaging studies have shown that cold-water VCS also consistently activates an endogenous highly conserved (>230 million years old) restorative-function network (Ngo & Kaplan, 2023) of predominantly contralateral structures including the anterior cingulate cortex (ACC), temporo-parietal areas (TPA; e.g., temporoparietal junction, superior temporal gyrus, inferior parietal lobe), middle frontal gyrus, insular cortex, thalamus & putamen (in basal ganglia). Correspondingly, the technique’s wide-ranging multimodal effects across mood, pain, cognition, attention, perception, beliefs/insight & mobility have been highlighted by remarkable therapeutic benefits shown in adults with often disabling refractory conditions such as nociplastic pain syndromes (e.g., phantom limb & post-stroke thalamic pain, migraine, CRPS/allodynia, spinal cord injury pain, refractory FM — Kaplan et al., 2024); other neurological disorders (e.g., Parkinson’s disease, minimally conscious state); and psychiatric illness (e.g., bipolar & schizophrenia spectrum disorders).
Figure 1: VCS with Caloric Irrigation — From Neurodiagnostic Technique to Therapeutic Neuromodulation Modality. The caloric test — via the vestibulo-ocular reflex — is a simple, low-cost, low-risk, non-invasive and widely used mainstream neurodiagnostic technique for balance problems & brain death, with a long-standing record of safety since its development over a century ago. The technique is routinely performed for example in primary care clinics by family doctors & nurses (for cerumen removal), audiologists, neurologists & ENT physicians. VCS involves irrigation of the external ear canal with warm/cold water (e.g., 1–4° C) while the head is reclined at 30° to the horizontal until nystagmus is observed and vertigo is reported — typically within a few seconds — via stimulation of semicircular canals & brainstem circuits (indicated by the black horizontal arrows). Over recent decades, several brain-imaging studies have shown that cold-water VCS also consistently activates an endogenous highly conserved (>230 million years old) restorative-function network (Ngo & Kaplan, 2023) of predominantly contralateral structures including the anterior cingulate cortex (ACC), temporo-parietal areas (TPA; e.g., temporoparietal junction, superior temporal gyrus, inferior parietal lobe), middle frontal gyrus, insular cortex, thalamus & putamen (in basal ganglia). Correspondingly, the technique’s wide-ranging multimodal effects across mood, pain, cognition, attention, perception, beliefs/insight & mobility have been highlighted by remarkable therapeutic benefits shown in adults with often disabling refractory conditions such as nociplastic pain syndromes (e.g., phantom limb & post-stroke thalamic pain, migraine, CRPS/allodynia, spinal cord injury pain, refractory FM — Kaplan et al., 2024); other neurological disorders (e.g., Parkinson’s disease, minimally conscious state); and psychiatric illness (e.g., bipolar & schizophrenia spectrum disorders).
.jpg) Figure 2. VCS Effects on Pain Measures & Percentage of Participants.
Figure 2. VCS Effects on Pain Measures & Percentage of Participants.
(A) Immediate Reduction in Pain Intensity after VCS. The box plot shows the distribution of pain intensity NRS ratings before (pre) and 30 minutes after (post) VCS where 0 = No pain and 10 = Worst pain imaginable. This analysis included participants who experienced at least a 4/10 pre-intervention NRS pain score (Nf27). A baseline level of at least 4/10 pain is the standard pain threshold used for inclusion in FM clinical trials. Pain scores were significantly reduced at 30 minutes following the procedure (t = -3.46, p = 0.002). P value is from a paired t-test of pre- and post-VCS pain scores. The bold horizontal bar in each box plot indicates the group’s mean pain intensity rating.
(B) Percentage of Participants with at least a 30% or 50% Improvement at 30 minutes and 24 hours after VCS. At 30min post-treatment, pain scores decreased by at least 30% in 8 (30%) participants and by at least 50% in 6 (22%) participants. Twenty-four hours after VCS, 11 participants (41%) experienced at least 30% decrease in pain and 10 participants (37%) experienced at least 50% decrease in pain. This analysis included participants who experienced at least a 4/10 pre-intervention NRS pain score (n = 27). The decision to exclude participants with less than 4/10 pain from this analysis was made post-hoc to avoid skewing percentages from participants with baseline scores of 2/10 pain, in which a one-point reduction on the pain scale represented a 50% decrease in pain.
(C) Reduction in pain intensity & pain interference (BPI-SF) 24 hours after VCS treatment. The box plots show distribution of BPI-SF pain intensity and pain interference scores for all study participants (n = 39). Paired t tests showed a significant reduction in pain intensity (t = -4.36, p = 0.0008) and pain interference scores (t = -3.67, p = 0.0001). The bold horizontal bar in each box plot indicates the respective group’s mean pain intensity & mean pain interference ratings.
.jpg) Figure 3. VCS Effects on Subjective Well-being & Autonomic Functioning
Figure 3. VCS Effects on Subjective Well-being & Autonomic Functioning
(A) Immediate Improvement in Subjective Well-Being after VCS. The box plots show the distribution of subjective well-being NRS ratings (0 = lowest quality of life; 10 = best quality of life imaginable) of all study participants (n = 39) before (pre) and 30 minutes after (post) VCS. Overall well-being ratings significantly improved post-procedure (t = 3.89, p < 0.001). P value is from paired t-test of pre- & post-VCS ratings.
(B) Autonomic Distress Improves for 1 to 4 weeks after VCS. The Composite Autonomic Symptom Score-31 (COMPASS-31) is a validated self-assessment tool used to evaluate the extent of distress secondary to autonomic symptoms. A repeated-measures ANOVA showed COMPASS 31 scores significantly improved over time (p < 0.001). Post-hoc comparisons using paired t-tests with Bonferroni correction revealed significant changes in the ME/CFS group (orange line) between baseline and all follow-up timepoints (1 week — t = -3.39, p.adj = 0.016; 2 weeks — t = -3.33, p.adj = 0.019; 4 weeks — t = -3.61, p.adj = 0.019). In the FM group (red line), significant effects were found between baseline and 1 week (t = -3.29, p.adj = 0.049). Beyond one-week post-intervention in the FM group, incomplete data limited our ability to assess the durability of these effects. Nevertheless, the current trial is the first study to demonstrate preliminary findings of VCS therapeutic effects on these autonomic functioning outcome measures in any clinical cohort. All study participants (Nf39) were included in analysis.
To cite this abstract in AMA style:
Kaplan M, Canori A, Howard R, Torkian T, Pietro R, Santiago-Pichardo G, Clauw D, Putrino D, Ali Y, Tabacof L, Ngo T. Vestibulocortical Stimulation via Caloric Irrigation in Nociplastic Disease: Therapeutic Effects on Pain, Autonomic Functioning & Quality of Life Measures [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/vestibulocortical-stimulation-via-caloric-irrigation-in-nociplastic-disease-therapeutic-effects-on-pain-autonomic-functioning-quality-of-life-measures/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/vestibulocortical-stimulation-via-caloric-irrigation-in-nociplastic-disease-therapeutic-effects-on-pain-autonomic-functioning-quality-of-life-measures/