Session Information
Date: Monday, October 27, 2025
Title: (1221–1247) Pain in Rheumatic Disease Including Fibromyalgia Poster
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Pain in patients with Systemic Lupus Erythematosus (SLE) is not well understood. There is role of active disease in pain (e.g. arthritis, serositis) also referred as Type I symptoms. Other factors e.g. coexistent fibromyalgia (FM), Stress, Fatigue, Sleep and Depression (Type 2 symptoms) may contribute towards pain.We undertook analyses of data on patients with SLE to better understand Pain using three different measures of Pain. We focused specifically on contribution/s of disease activity, FM, Sleep, Stress, Depression and Fatigue.
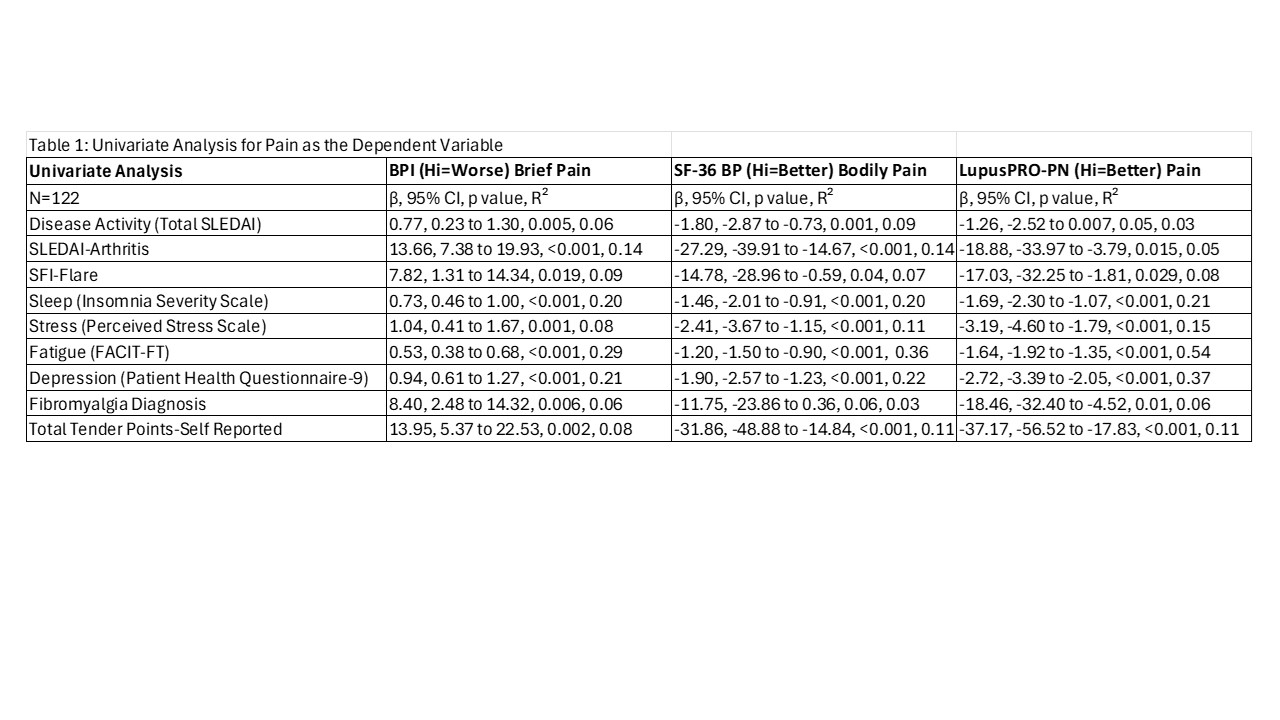
Methods: Cross-sectional Data from 122 SLE patients meeting the 1997 ACR classification criteria were analyzed. Pain was measured using Brief Pain Inventory (BPI), SF-36 Bodily Pain (BP) and LupusPRO Pain domain. Disease activity and Flare were measured using SELENA-SLEDAI and SFI. Tools to measure Sleep, Fatigue, Stress, Depression were the Insomnia Severity Index, FACIT-FT, Perceived Stress Scale-PSS and Patient Health Questionnaire-9/PHQ9. FM status was determined by chart review and patient reported tender point count. We conducted univariate regression analyses with Pain as the dependent variable and others as independent variables. We next undertook multivariate analyses of significant variables from the univariate analysis (Model 1), with FM (Model 2), and stepwise regression analysis (Model 3). We show chart-based FM results below. Results were similar for tender point counts.
Results: 90% were women; 51% Black, 23% White, 12% Hispanic and 9% Asian. Mean age was 40.7 (13.5) yrs, with Mean (SD) SLEDAI 5.03 (4.0) and SDI 0.61 (0.96). Mean Disease duration was 8.6 (7.2) years. 33% had SFI flare, and 63% were on steroids. 16% had FM. There was a good correlation between the three pain measures (r >0.65). Mean (SD) BPI, BP and PRO-Pain were 11.98 (12.29), 58.71 (24.7) and 69.80 (28.16).Disease activity (including SLEDAI-arthritis and SFI), Sleep, Stress, Fatigue, Depression and Fibromyalgia were associated with Pain (Table 1) on univariate analysis. On multivariate analysis (Table 2) disease activity, sleep, fatigue and depression were associated with Pain after adjusting for all other variables (R² 60-70%) %, and the associations were not changed significantly by adding FM to the model. On Stepwise Regression, 3-4 variables explained 56-68% of variance in Pain (Table 2), with disease activity being associated in all the three measures of Pain. In addition, sleep, depression and fatigue were associated with Pain, but not FM or stress.
Conclusion: Pain in SLE is associated with active disease. Latter, along with sleep, fatigue and depression explains more than half of the pain in SLE, indicating that besides controlling disease activity, there may be a role for Biopsychosocial model of care in improving pain in SLE. These models report association and not causation. Longitudinal study models will be tested next.
.jpg)
To cite this abstract in AMA style:
Jolly M. Demystifying Pain in patients with Lupus: How much is it Lupus and How much is it Other Stuff? [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/demystifying-pain-in-patients-with-lupus-how-much-is-it-lupus-and-how-much-is-it-other-stuff/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/demystifying-pain-in-patients-with-lupus-how-much-is-it-lupus-and-how-much-is-it-other-stuff/