Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: RA requires resource-intense management, with a joint exam recommended every 3-6 months to monitor disease activity. Frequent in-person visits are burdensome for patients and exacerbate access issues, contributing to long wait times and suboptimal care. Up to half of RA patients receive virtual rheumatology care, which can improve access and treatment adherence when added to office care. We know little about virtual care practices of RA management and how they compare to in-office practices. We aim to compare documentation of disease activity measure (DAM) assessment and treatment changes at virtual vs in-office RA visits in a large academic health system.
Methods: We conducted a retrospective cross-sectional study of a convenience sample of RA patients seen at University of Michigan rheumatology clinic from 2021-2024. We required a) a documented RA diagnosis in a clinical note by an attending rheumatologist during the study period, b) ≥1 office and ≥1 virtual visit during the study period to limit selection bias by disease activity/severity. We extracted patient- and visit-level data from the electronic medical record using a standardized collection form. We used descriptive statistics to evaluate a) patient-level characteristics stratified by virtual care utilization (at/below vs above the mean ratio of virtual to total visits), b) visit-level documentation of disease activity measures (DAMs) and DMARD or glucocorticoid (GC) changes.
Results: We reviewed 330 visit notes (111 virtual, 219 office) for 64 RA patients seen by 3 rheumatology attendings during the study period. At the patient level, median (IQR) office and virtual visit counts were 1 (1-2) and 4 (2-4) respectively (Table 1). Mean (SD) virtual care utilization was 0.34 (0.16) and similar across attendings. Demographics and rheumatology clinic contact were similar across levels of virtual care utilization. Patients with higher virtual care utilization had higher rates of fibromyalgia (3.2 vs 9.0%, p < 0.0001), seropositivity (80.7 vs 87.9%, p < 0.0001), RA duration (median 14 vs 21 years, p 0.0002), and TNF inhibitor use (54.8 vs 30.3%, p 0.05). All attendings were less likely to document DAMs at virtual vs. office visits (p < 0.0001) (Table 2). Patient-reported DAM documentation was low in both settings (total N = 1). We saw significant between-provider differences in joint count documentation at both virtual and office visits, inflammatory marker and treatment change documentation at virtual visits (p 0.004 DMARD, 0.005 GC), and DMARD change documentation at office visits (P 0.038). Attending 3 was less likely to change treatment at virtual vs in-office visits (p 0.05); documentation was consistent across settings for attendings 1 and 2 (all p ≥0.1).
Conclusion: In a sample of RA patients seen both virtually and in-office, we saw variation in DAM and treatment change documentation a) between settings across attendings, b) across attendings in each setting. Patient-reported DAM collection was low overall. Further work is needed to confirm these findings, and to develop and test provider-facing interventions to improve DAM collection and treatment optimization in the virtual setting.
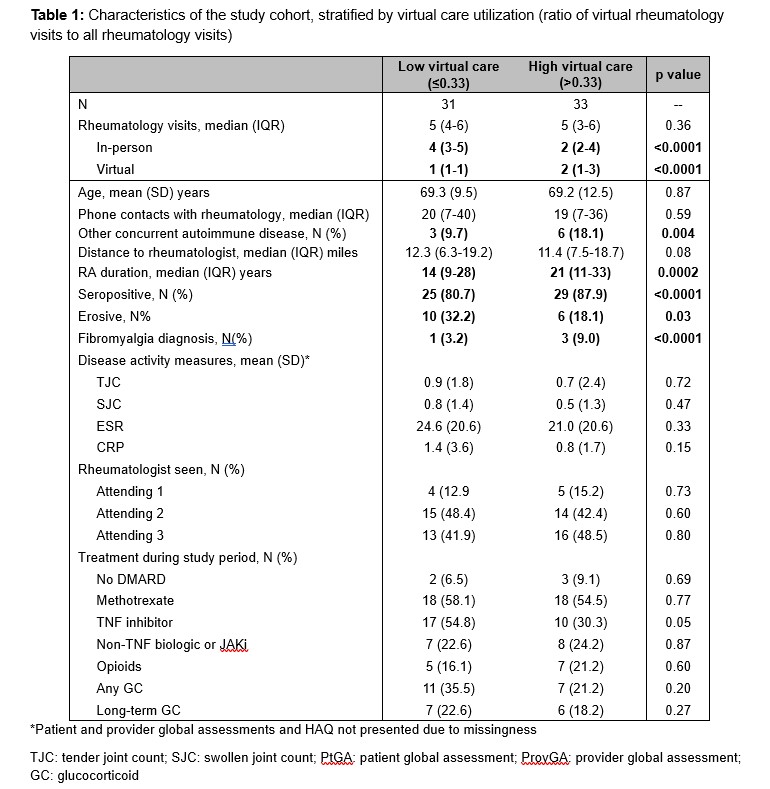 Table 1: Characteristics of the study cohort, stratified by virtual care utilization (ratio of virtual rheumatology visits to all rheumatology visits)
Table 1: Characteristics of the study cohort, stratified by virtual care utilization (ratio of virtual rheumatology visits to all rheumatology visits)
.jpg) Table 2: Virtual and office disease activity and treatment change documentation, stratified by treating rheumatologist
Table 2: Virtual and office disease activity and treatment change documentation, stratified by treating rheumatologist
To cite this abstract in AMA style:
Khader Y, Bautista Sanchez R, Kelekar A, Kerski M, Wallace D, Dickinson O, Cohen-Mekelburg S, England B, Baker J, Cannon G, Clauw D, Wallace B. Variation in RA disease activity measure assessment and treatment change documentation in virtual vs in-office rheumatology visits [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/variation-in-ra-disease-activity-measure-assessment-and-treatment-change-documentation-in-virtual-vs-in-office-rheumatology-visits/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/variation-in-ra-disease-activity-measure-assessment-and-treatment-change-documentation-in-virtual-vs-in-office-rheumatology-visits/