Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Idiopathic recurrent pericarditis (IRP) is characterized by recurrent pericarditis attacks, and autoinflammatory pattern has been highlighted due to similarities in both clinical features and treatment responses. The most feared complication of recurrent pericarditis is constrictive pericarditis (CP), with a very low risk in IRP patients on conventional treatment but higher in those who are corticosteroid-dependent and colchicine-resistant.
Persistent pericardial effusion in patients with clinical remission is another concern, with a small proportion of those under conventional treatment showing mild, ongoing effusion on echocardiography. However, data on long-term echocardiographic findings in IRP patients who are resistant to conventional treatment and require Anakinra therapy are limited.
In this study, we aimed to evaluate pericardial thickness, pericardial echogenicity, pericardial effusion, and the presence of tamponade and CP using echocardiography in IRP patients treated with Anakinra.
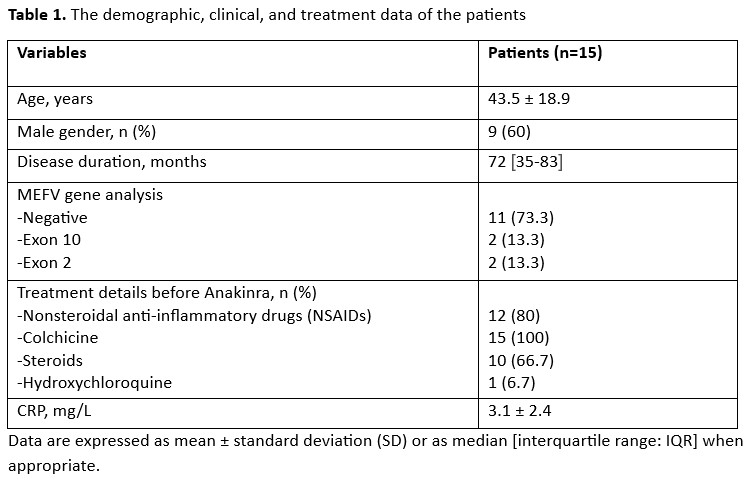
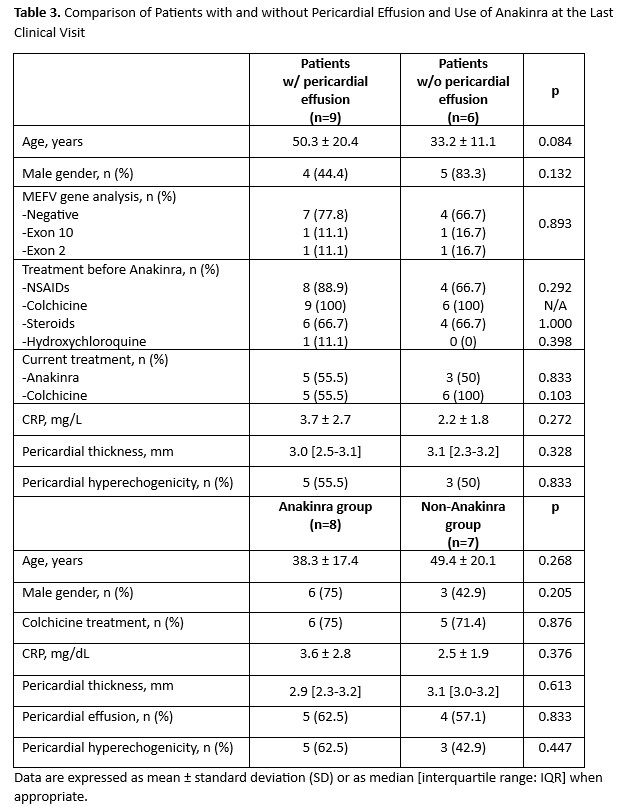
Methods: We recruited 15 patients with IRP who had been treated with Anakinra at our autoinflammatory clinic between 2011 and 2023 and had been in clinical and laboratory remission for the past three months. All patients had echocardiographic data available within the last three months. Demographic, clinical, and treatment data were extracted from patient records. Echocardiographic data were compared with age- and gender-matched healthy controls (HC). Additionally, patients were stratified into two groups: those who had discontinued Anakinra treatment and those who were continuing the treatment. Furthermore, to understand the persistence of pericardial effusion despite clinical remission, patients with pericardial effusion were compared with those without effusion.
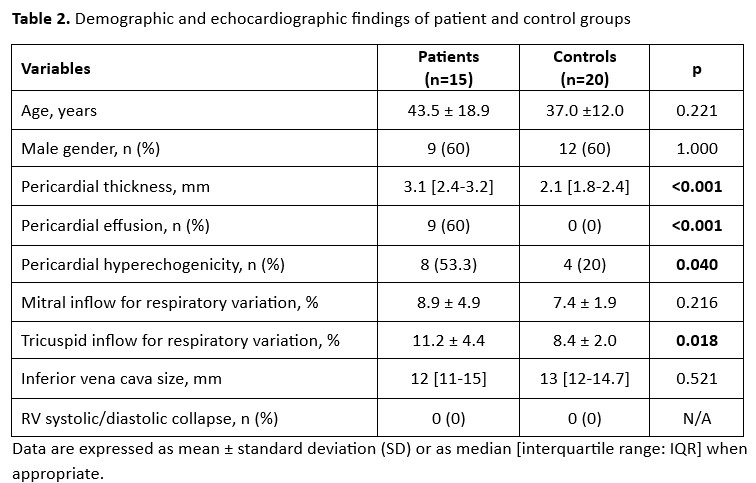
Results: Fifteen IRP patients and 20 HC were included in the study. The demographic, clinical, and treatment data of the patients are shown in Table 1. Echocardiographic examination revealed that pericardial thickness and hyperechogenicity were significantly higher in patients than HC (p< 0.001). Mild pericardial effusion (< 10 mm) persisted in 60% of the patients. No patients had pericardial tamponade or constrictive pericarditis. However, tricuspid inflow for respiratory variation was significantly higher in the patient group than in HC (p=0.018) (Table 2). No significant differences were observed in the variables between patients continuing Anakinra treatment and those who had discontinued it, and there were also no differences between patients with pericardial effusion and those without effusion (Table 3).
Conclusion: We found that IRP patients treated with Anakinra and in remission had greater pericardial thickness and hyperechogenicity than HC, and most still had mild effusion. It is unclear whether these findings are sequelae of past pericarditis or signs of subclinical ongoing inflammation. Although tamponade and constrictive pericarditis were not detected, the significantly higher tricuspid inflow for respiratory variation, an early sign of tamponade, compared to controls is noteworthy. Therefore, these patients should be closely monitored to identify and manage potential complications.
To cite this abstract in AMA style:
Toker Dincer Z, Raimoglu D, Yilmaz E, Dag A, Karup S, Melikoglu M, Ugurlu S. Long-Term Echocardiographic Findings in Idiopathic Recurrent Pericarditis Patients Treated with Anakinra [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/long-term-echocardiographic-findings-in-idiopathic-recurrent-pericarditis-patients-treated-with-anakinra/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/long-term-echocardiographic-findings-in-idiopathic-recurrent-pericarditis-patients-treated-with-anakinra/