Session Information
Session Type: Abstract Session
Session Time: 4:00PM-5:30PM
Background/Purpose: VEXAS (Vacuoles, E1 Enzyme, X-Linked, Autoinflammatory, Somatic) syndrome is an autoinflammatory monogenic disease caused by inactivating somatic mutations in the UBA1 gene and characterized by heterogenous systemic auto-inflammation and progressive hematologic manifestations. Its management is not consensual but often include biologic DMARDs or azacytidine in case of association with myelodysplastic syndrome. Prognosis appears to be poor, with substantial morbidity and mortality mainly caused by infection. The aim of this study was to describe the spectrum of infectious complications and their risk factors in VEXAS patients.
Methods: Retrospective multicenter study including patients with genetically proven VEXAS syndrome, with at least one episode of severe infection (defined as an infection leading to hospitalization and/or intravenous infectious treatments and/or death). These patients were compared to a cohort of 50 VEXAS patients without severe infection after at least one year of follow-up since diagnosis. Risk factors of infections were assessed with multivariate Cox proportional hazard ratios models.
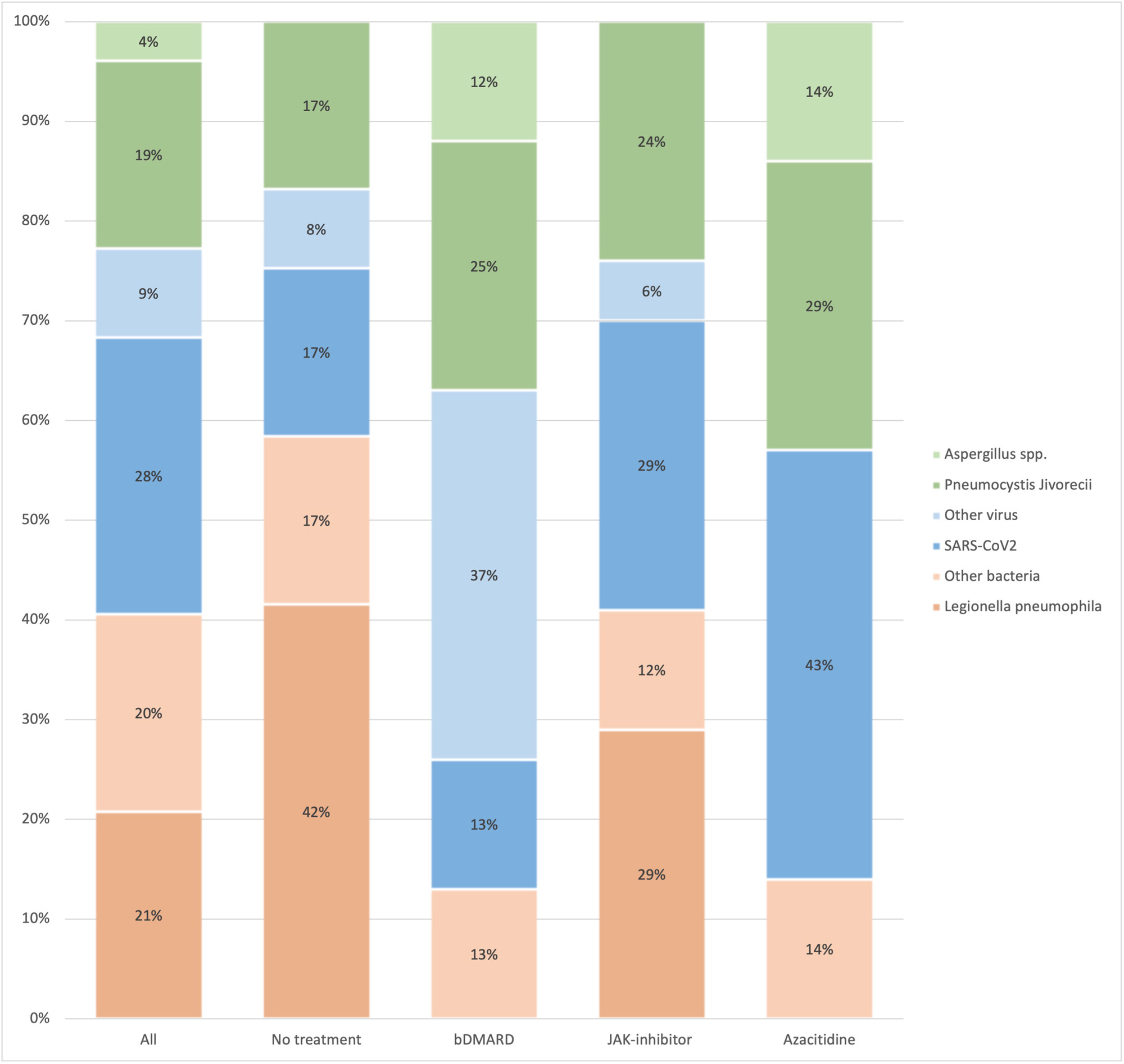
Results: Seventy-four patients (99% male, median [IQR] age at VEXAS onset of 68 [63-75] years) with 133 severe infections were included. Infections occurred despite anti-infective prophylaxis in 46% of cases. The main immunosuppressive drugs received at the time of infection were JAK inhibitors (29%), biologics (21%) and azacitidine (11%), while 16% of infections occurred without treatment (no immunosuppressant or corticosteroids ≤ 10 mg/d). Most frequent infection localizations were the lung (59%), skin (10%) and urinary tract (9%). The most commonly found infectious agents were SARS-CoV-2, Legionella pneumophila and Pneumocystis jivoreci in 28%, 21% and 19% of pulmonary infections, respectively (figure 1).Invasive fungal infections accounted for 11% of all infections. Nearly 20% of pulmonary infections occurred in the absence of treatment with a high prevalence of L. pneumophila (42%) and P. jivoreci (17%) infections.
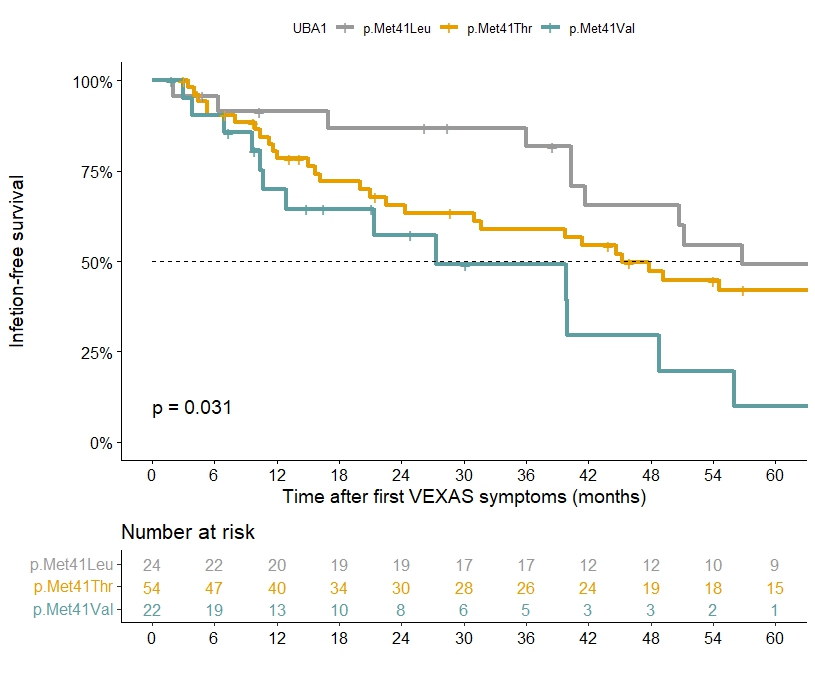
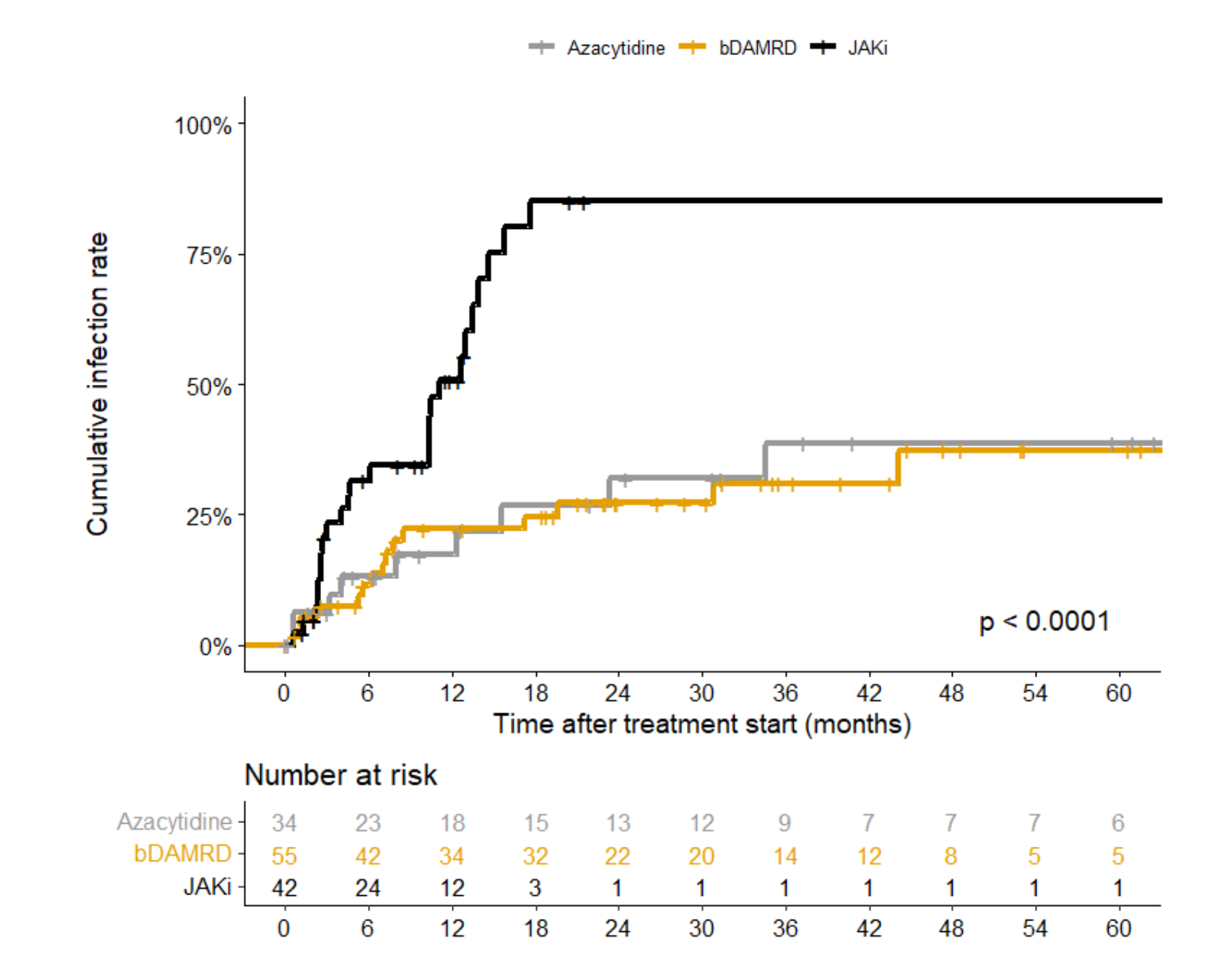
In multivariate analysis, factors significantly associated with severe infection were p.Met41Val mutation (figure 2) (HR 2.44 [1.05-5.63], p=0.037), age at symptom onset >75 years (HR 1.91 [1.05-3.47], p=0.034) and arthralgia (HR 2.03 [1.16-3.56], p=0.013) whereas leukopenia was a protective factor (HR 0.58 [0.34-0.99], p=0.046). Among treated patients, cumulative infection rate was significantly higher with JAK inhibitors (multivariate HR 3.90 [1.78-8.55], p=0.001) compared to biologic DMARDs and azacitidine, with a median time to infection of 12 months (figure 3). After a median follow-up of 4.4 [2.5–7.7] years, 27 (36%) patients died including 15 (56%) due to severe infection.
Conclusion: VEXAS syndrome is associated with a high incidence of severe infections especially in patients carrying the p.Met41Val mutation. The high frequency of atypical infections such as legionellosis and invasive fungal infections in patient without immunosuppressive treatment might suggest an intrinsic immunodeficiency of the disease. JAK inhibitors, used as first-line treatment, are particularly at risk of severe infections occurring early after initiation.
To cite this abstract in AMA style:
de Valence de Minardiere B, Delaune M, Nguyen Y, Jachiet V, Heiblig M, Jean A, Henneton P, Riescher-tuczkiewicz s, Guilpain P, Lobbes H, Le Guenno G, Schleinitz N, Lacombe V, Langlois V, Outh R, Vinit J, Martellosio J, Decker P, Vlakos A, Moulinet T, Dieudonne Y, Bigot A, Terriou L, De Maleprade B, Denis G, Broner J, Kostine M, Humbert S, Terrier B, Georgin-Lavialle S, Fain O, Mekinian A, MORGAND M, Comont T, Hadjadj J. Severe Infections in Patients with VEXAS Syndrome: A Study from the French VEXAS Group [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/severe-infections-in-patients-with-vexas-syndrome-a-study-from-the-french-vexas-group/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/severe-infections-in-patients-with-vexas-syndrome-a-study-from-the-french-vexas-group/