Session Information
Date: Monday, November 14, 2022
Title: SLE – Diagnosis, Manifestations, and Outcomes Poster III: Outcomes
Session Type: Poster Session D
Session Time: 1:00PM-3:00PM
Background/Purpose: The complement system is a key-player in the pathogenesis of systemic lupus erythematosus (SLE); decrease in C3 and C4 levels correlates with disease activity and precedes clinically evident flare. Since synthesis of complement proteins increase during gestational course, it is debated whether complement levels exert a prognostic role in pregnant women with SLE.
We performed a network meta-analysis to assess the prognostic role of complement in pregnant SLE women, to evaluate the possible role of complement fluctuations during pregnancies.
Methods: Data from available prospective studies (Jan 2002-Dec 2020) investigating pregnancies in at least 50 SLE patients, excluding miscarriages before 12 weeks, werepooled together. After a systematic literature search, corresponding authors of 19 retrieved studies meetinginclusion criteria were invited to contribute with additional data, including complement C3 and C4 levels [6 months before pregnancy, at conception, 1st trimester (T1), 2nd trimester (T2), 3rd trimester (T3) and 3 months after delivery].
Results: A total of 532 SLE women from four eligible studies were included in the analysis [1-4]. Lupus Nephritis (LN) was diagnosed in 237 patients (44.5%) and Antiphospholipid Syndrome in 68 (12.8%). A total of 170 patients (32%) experienced a flare during pregnancy, defined as need of new Immunosuppressants or increase of prednisone > 9 mg/day.
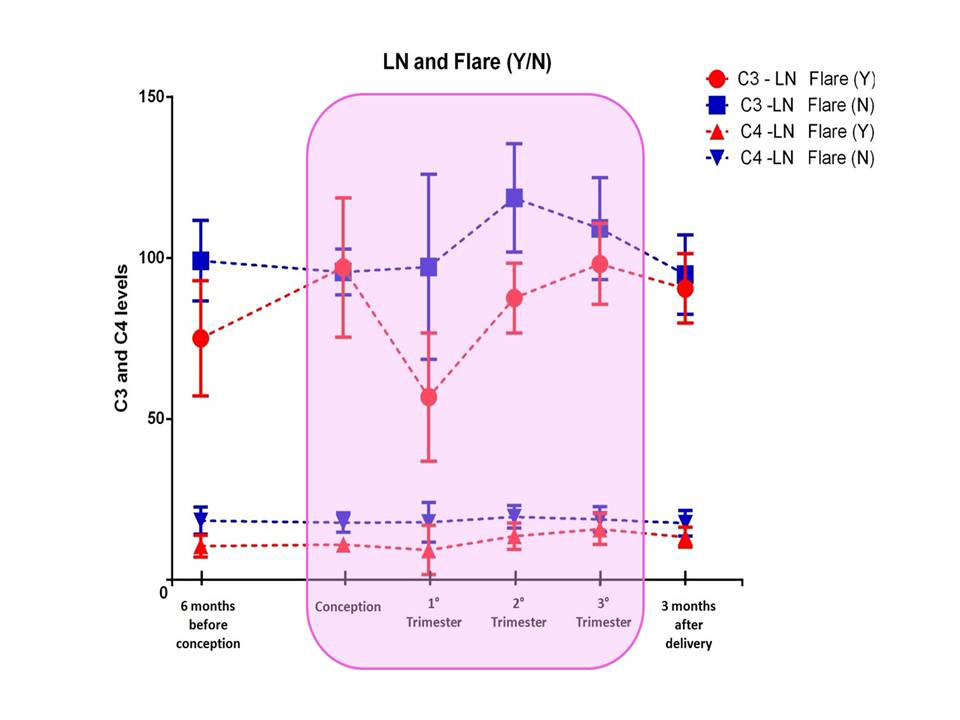
Patients with LN had significantly lower mean levels of complement (C3 at conception; C3 at T1; C3 after 3 months of delivery; C4 at all timepoints except for C4 at T3). SLE patients who experienced flares during pregnancy had significantly lower mean levels of complement (all timepoints for both C3 and C4). Table 1 shows the mean C3 and C4 levels in different timepoints according to diagnosis and flare during pregnancy. Pregnancies with flare had a higher rate of maternal of fetal complications (60% vs.50.3%;p=0.03). The lowest levels of complement were observed in patients with a concomitant diagnosis of LN and presence of flare, particularly during theT1 (Figure 1). Nevertheless, both in LN and flare groups the lowest levels of C3 and C4 were documented at T1.
Conclusion: In this prospective large cohort of SLE patients low C3/C4 levels, particularly in T1, were associated with a higher frequency of flare. Lowering levels of complement, especially in T1, even within normal range might alert the treating clinicians in predicting disease course and consequently avoid flares, especially in LN.
To cite this abstract in AMA style:
Radin M, Cecchi I, Crisafulli F, Klumb E, De Jesús G, Saavedra M, Reyes-Navarro G, iaccarino L, Larosa M, Moroni G, Tamborini F, Roccatello d, Andreoli L, Chighizola C, Sciascia S. A Network Meta-analysis on 532 SLE Patients: Low Complement Levels in the First Trimester Predict Disease Flare in Pregnancy [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/a-network-meta-analysis-on-532-sle-patients-low-complement-levels-in-the-first-trimester-predict-disease-flare-in-pregnancy/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-network-meta-analysis-on-532-sle-patients-low-complement-levels-in-the-first-trimester-predict-disease-flare-in-pregnancy/