Session Information
Date: Sunday, November 13, 2022
Title: Abstracts: SLE – Diagnosis, Manifestations, and Outcomes II: Complications
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: Infections are a major cause of morbidity and mortality in systemic lupus erythematosus (SLE). We assessed the incidence and risk factors for major infections in adult SLE.
Methods: We carried out a retrospective review of 1354 patients of SLE (ACR 1997 criteria) with age ≥18 years visiting the rheumatology clinic at a single centre between 2000 to 2020. Clinical details were retrieved from clinical case records and supplemented with data from the hospital electronic health records. Serious infection was defined as the need for hospitalization, or infection resulting in disability or death. Cox regression was used to determine factors associated with a serious infection and the effect of each serious infection on overall survival.
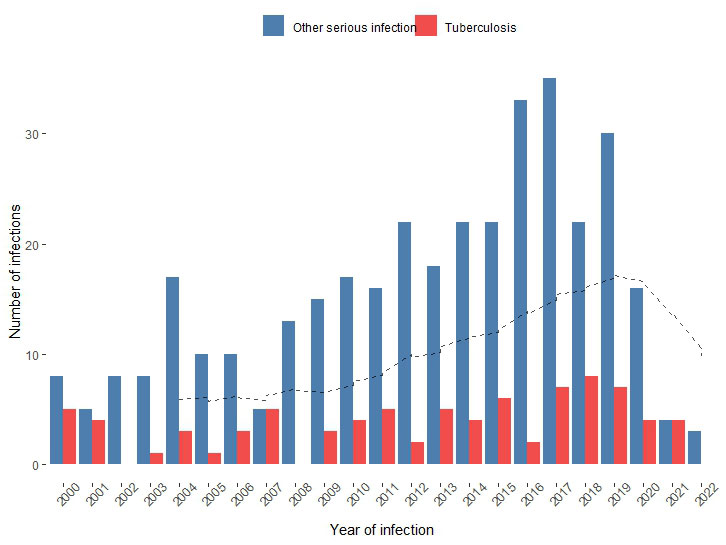
Results: Among the 1354 patients (1258 females) with a mean age of 30.32 ±9.42 years and a cumulative follow up of 7127.89 person-years. A total of 439 major infections occurred in 339 (25.03% of the cohort) individuals at a rate of 61.6 serious infections per 1000 person-years of follow-up. Recurrent infections occurred in 101 (7.45%) patients. The average number of infections increased from 9.9 to 23.7 per year from 2000-09 to 2010-19.
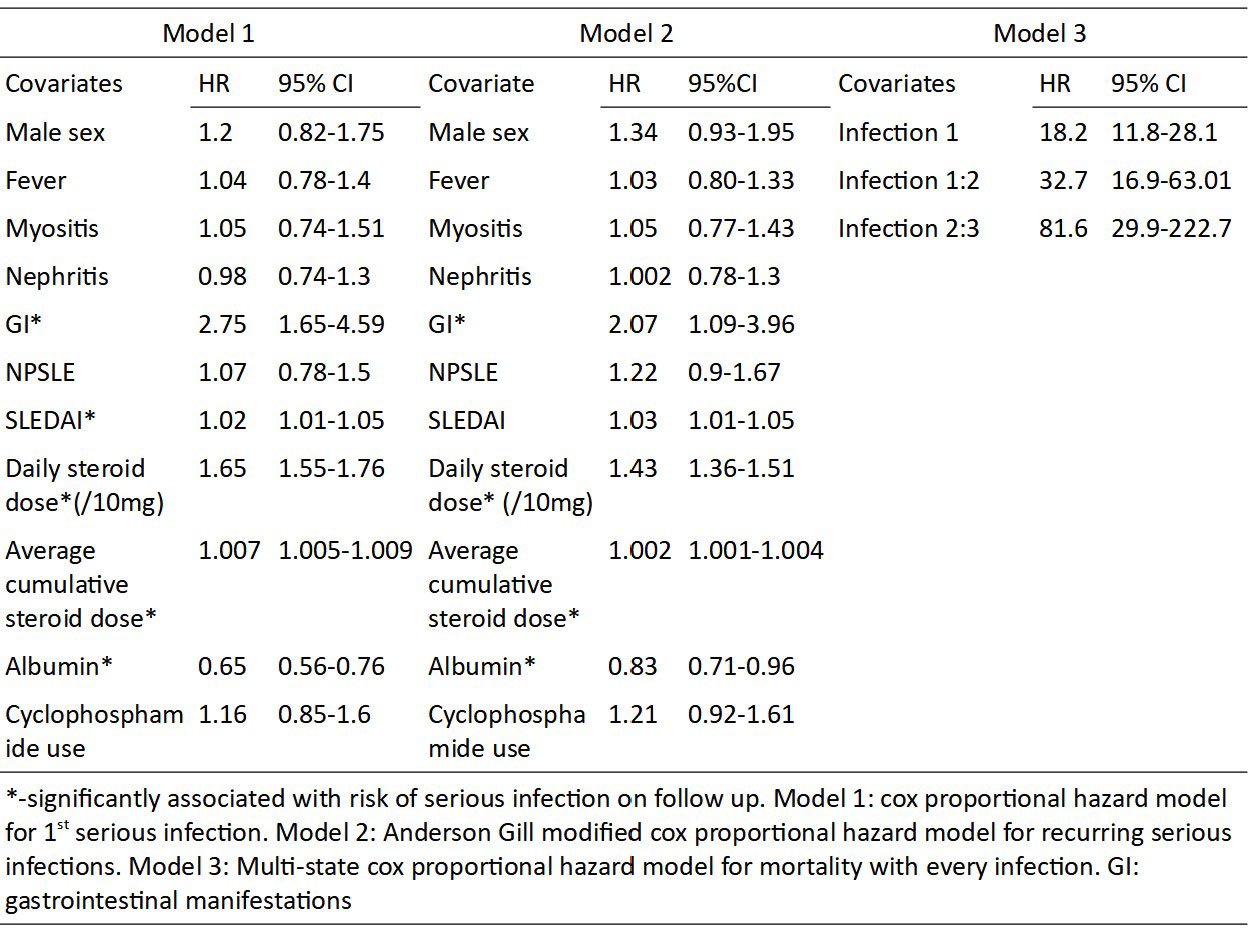
Among the microbiologically confirmed cases (79.9% of cases) Tuberculosis (81) was the most common organism followed by S. aureus (65), E. coli (51), K. pneumoniae (29), P. aeruginosa (29), S. pneumoniae (20), Acinetobacter spp. (9), E. fecalis (9), Nocardia (4), Salmonella (3), Proteus (1) and Listeria (1). Forty (9.1%) opportunistic infections occurred: Cytomegalovirus (11), disseminated Herpes zoster (10), invasive candidiasis (5), cryptococcal meningitis (5), histoplasmosis (2), and 1 each of Aspergillus flavus pneumonia, CNS toxoplasmosis and Giardia lamblia. On multivariate analysis SLEDAI-2K(HR 1.02, 1.01-1.05), gastrointestinal involvement (HR 2.75, 1.65-4.69), current steroid dose (HR 1.65,1.55-1.76), average cumulative steroid dose per year (HR 1.007, 1.005-1.009) were associated with serious infection and higher albumin (HR 0.65, 0.56-0.76) was protective.
Serious infection led to more damage accrual (1 vs 0). Serious infection-free survival at 1 year and 5 years was 82.9% (80.8-85) and 73.8% (71.1-76.6). There were 119 deaths with infection attributable mortality in 65 (54.6%). Hazard ratio for mortality was 18.2, 32.7, and 81.6 for the first, second, and third serious infection.
Conclusion: Serious infections remain a major cause of mortality and damage accrual in SLE and are associated with higher disease activity, gastrointestinal involvement, hypoalbuminemia, current and cumulative steroid dose. TB prophylaxis in patients with SLE should be considered in endemic areas, especially when using high-dose steroid therapy.
To cite this abstract in AMA style:
Chatterjee R, Pattanaik S, Misra D, Agarwal V, Lawrence A, Aggarwal A. Serious Infections in SLE- Incidence, Associated Factors, Impact and Trends over Two Decades [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/serious-infections-in-sle-incidence-associated-factors-impact-and-trends-over-two-decades/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/serious-infections-in-sle-incidence-associated-factors-impact-and-trends-over-two-decades/