Session Information
Title: Systemic Sclerosis, Fibrosing Syndromes, and Raynaud’s - Clinical Aspects and Therapeutics II
Session Type: Abstract Submissions (ACR)
Background/Purpose: Pumonary hypertension (PH) is a significant complication of systemic sclerosis (SSc), with prevalence reports of 10-25%. Predictors of PH remain somewhat elusive. Our objective was to assess the pattern of PH timing and subtype development in limited versus diffuse cutaneous SSc.
Methods: From our prospectively enrolled institutional scleroderma databank we performed a 10-year cross-sectional study of consecutive patients seen between January 1, 2000 and December 31, 2009. PH was defined as a mean pulmonary artery pressure (PAP) > 25 mmHg on right heart catheterization (RHC) or transthoracic echocardiogram (TTE) with PAP > 45 and PH diagnosed by a cardiologist. Descriptive statistics were used for baseline and PH characteristics, Kaplan Meier plots for time to development of PH and Cox proportional hazards for adjusted analysis.
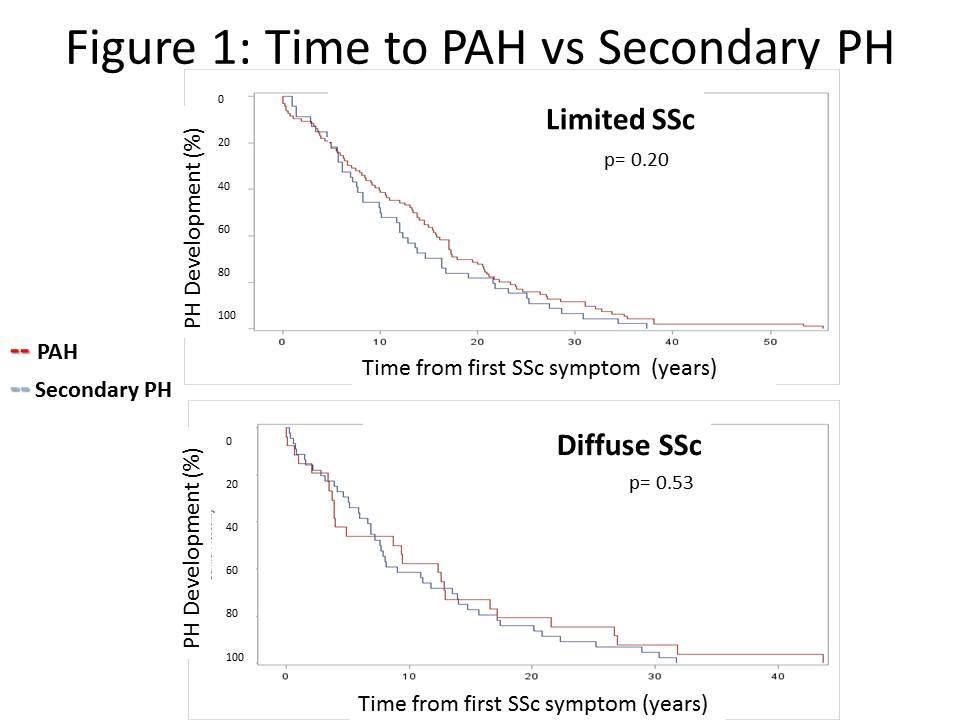
Results: Of the 1,156 SSc patients included, 80% were female, the average age at first SSc symptom was 43.7 ± 14.2 years, and 44% had diffuse SSc. Two hundred thirteen (18%) had PH, of whom 122 (10% of total) had pulmonary arterial hypertension (PAH) and 90 (8% of total) had PH secondary to either ILD (PH-ILD) or cardiac involvement (PH-cardiac). 75% were confirmed by RHC; 25% did not have available RHC numbers in the hospital system but were confirmed as PH by cardiology evaluation. Prevalence of all PH was more common in limited (22%) vs diffuse SSc (14%; p=0.001). The profile of PH subtype was different, with 67% of limited SSc having PAH, compared to 37% in diffuse SSc (p < 0.0001). As shown in Table 1 approximately 5% of diffuse patients developed PAH with more secondary PH, whereas limited SSc patients developed predominantly PAH (p=< 0.0001). Patients with limited SSc developed all PH later in disease at a median 12.0 (IQR 5.7, 20.7), compared to 7.7 (3.5, 14.7) years since first SSc symptom in diffuse SSc (p=0.02), and this persisted after adjustment for age and gender (p=0.02). However there was no difference in the time to development of PAH compared to secondary PH in either diffuse or limited SSc (Figure 1).
Table 1: Prevalence of PH subtypes in limited and diffuse SSc
|
|
Secondary PH |
|||
|
|
No PH |
PAH |
PH-ILD |
PH-cardiac |
|
Limited cutaneous SSc |
78% |
15% |
5% |
2% |
|
Diffuse cutaneous SSc |
86% |
5% |
6% |
3% |
Conclusion: These data suggest that although patients with limited SSc are more likely to develop PAH, the rate of PAH and secondary PH development is similar regardless of clinical subset. All SSc patients, including late diffuse SSc, should continue to be screened for all types of PH.
Disclosure:
M. Mohile,
None;
M. Lucas,
None;
V. D. Steen,
Gilead Science, ,
2,
Gilead Science,
5,
Actelion Pharmaceuticals US,
2,
Actelion Pharmaceuticals US,
8,
Roche Pharmaceuticals,
2,
Celgene,
2,
Sanofi-Aventis Pharmaceutical,
2;
T. A. Medsger Jr.,
None;
R. T. Domsic,
Actelion Pharmaceuticals US,
5.
« Back to 2013 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/pulmonary-hypertension-in-systemic-sclerosis-clinical-classification-and-pulmonary-hypertension-subtypes/